
Optics and Refraction — MCQs

On this page
Which of the following statements is correct regarding indirect ophthalmoscopy?
A 6-year-old child presents with a refractive error of -2D in the right eye and +1D in the left eye. Visual acuity is normal in both eyes with correction, and fundus examination reveals normal retinal findings. What is the most likely diagnosis?
The instrument shown below is:

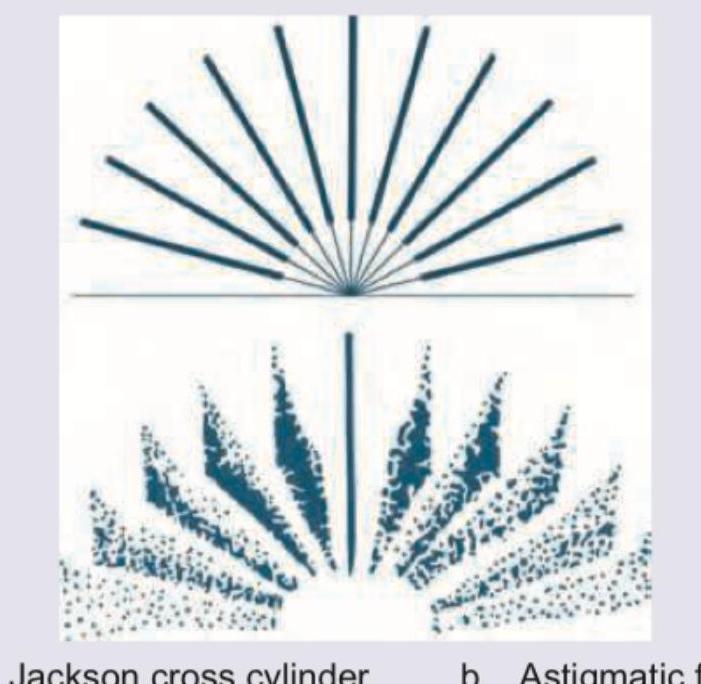
The following image shows:
The following image shows:
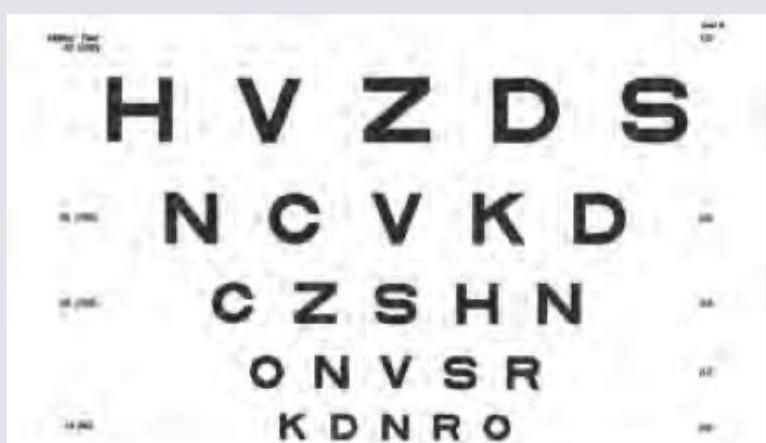
The image shows which chart for visual acuity?
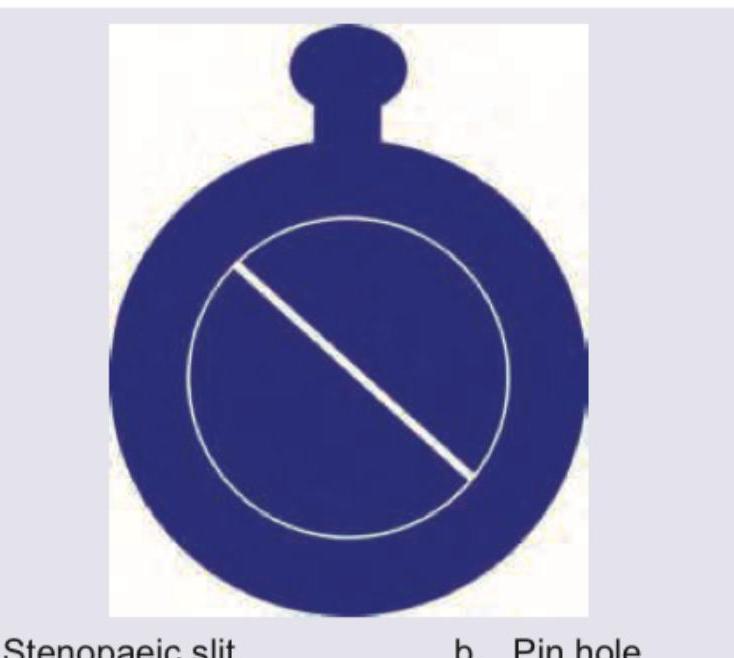
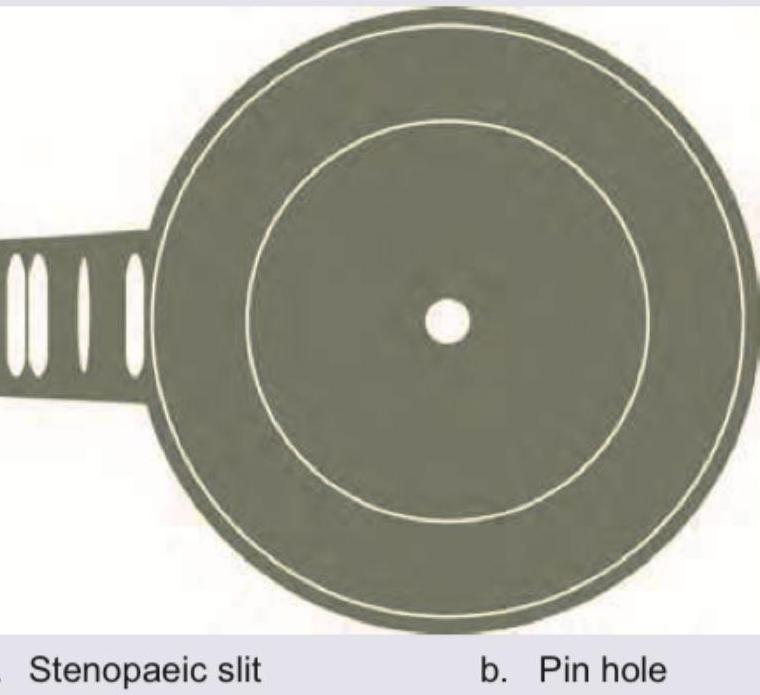
Which instruments are shown below?
All are true about the instrument shown except:

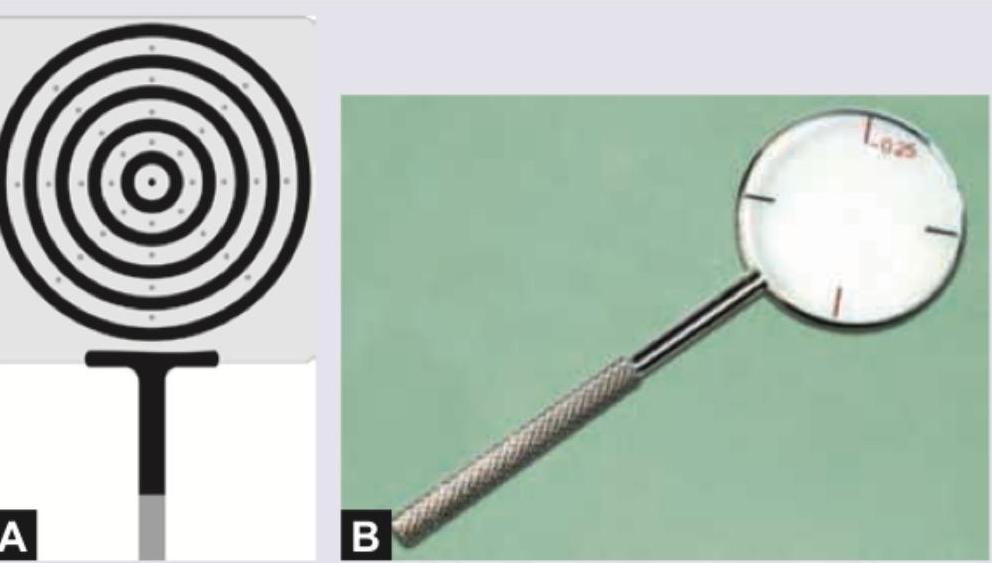
Name the instrument shown in the image:

What does the given image show?
Practice by Chapter
Physical Optics
Practice Questions
Geometric Optics
Practice Questions
Optical System of Eye
Practice Questions
Visual Acuity and Contrast Sensitivity
Practice Questions
Refractive Errors
Practice Questions
Accommodation and Presbyopia
Practice Questions
Optical Instruments
Practice Questions
Lenses and Prisms
Practice Questions
Retinoscopy
Practice Questions
Subjective Refraction
Practice Questions
Contact Lens Optics
Practice Questions
Wavefront Technology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app