
Optics and Refraction — MCQs

On this page
This instrument is used for :
What is the expected amplitude of accommodation in a healthy child?
A 58-year-old male presents with gradual painless visual field loss over several years. His intraocular pressure is 26 mmHg in both eyes. He has no history of ocular trauma or steroid use. Visual field testing reveals an arcuate scotoma in the superior field of the right eye. The optic disc of the right eye is shown in Image 2. Which structural finding visible in this image best explains the superior arcuate scotoma?

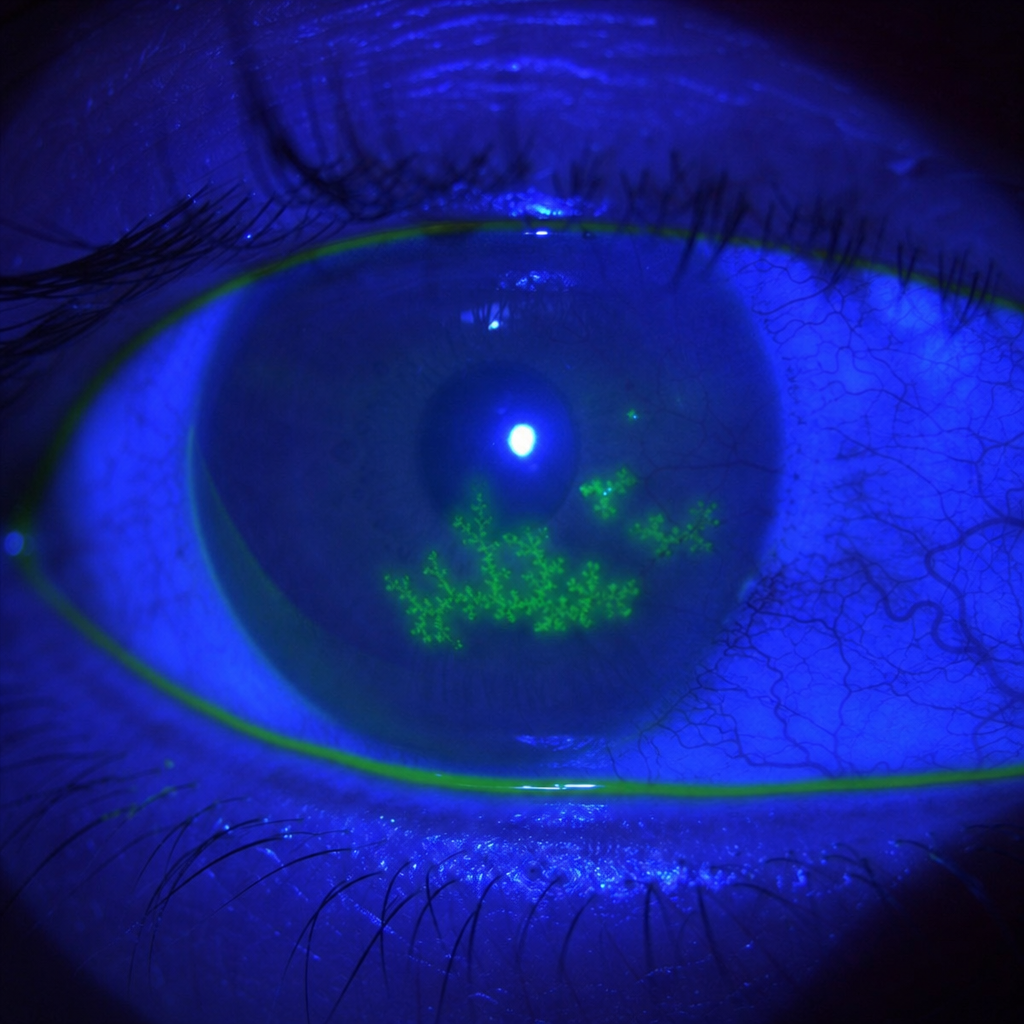
A 28-year-old man presents with a 3-day history of unilateral red eye, photophobia, and foreign body sensation. He had a similar episode 18 months ago that resolved with topical treatment. His visual acuity is 6/12 in the affected eye. The slit-lamp appearance under cobalt-blue light after fluorescein instillation is shown (Image 2). Which of the following is the most appropriate first-line topical treatment?
For refraction in a hypermetropic child, which is the best drug?
Practice by Chapter
Physical Optics
Practice Questions
Geometric Optics
Practice Questions
Optical System of Eye
Practice Questions
Visual Acuity and Contrast Sensitivity
Practice Questions
Refractive Errors
Practice Questions
Accommodation and Presbyopia
Practice Questions
Optical Instruments
Practice Questions
Lenses and Prisms
Practice Questions
Retinoscopy
Practice Questions
Subjective Refraction
Practice Questions
Contact Lens Optics
Practice Questions
Wavefront Technology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app