
Ophthalmic Surgery — MCQs

On this page
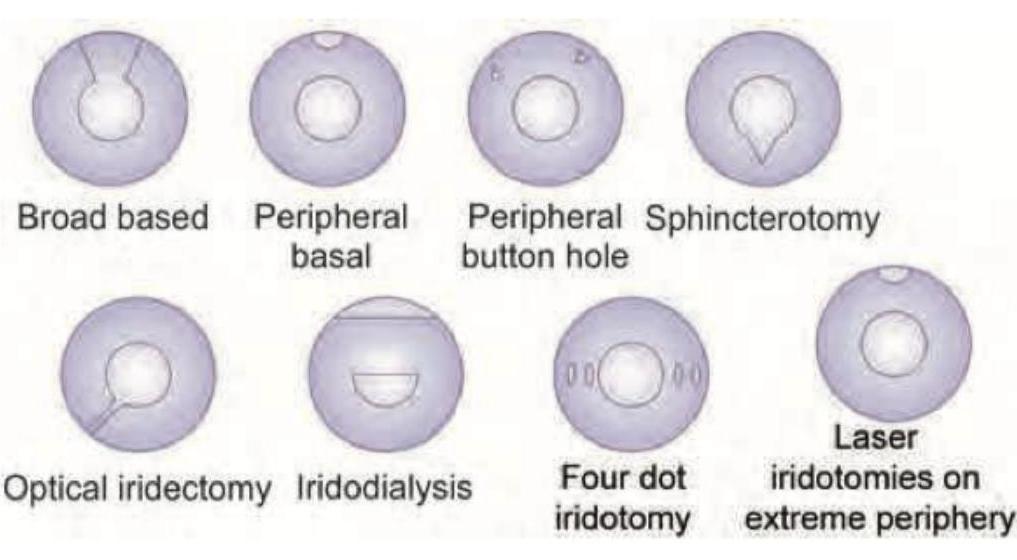
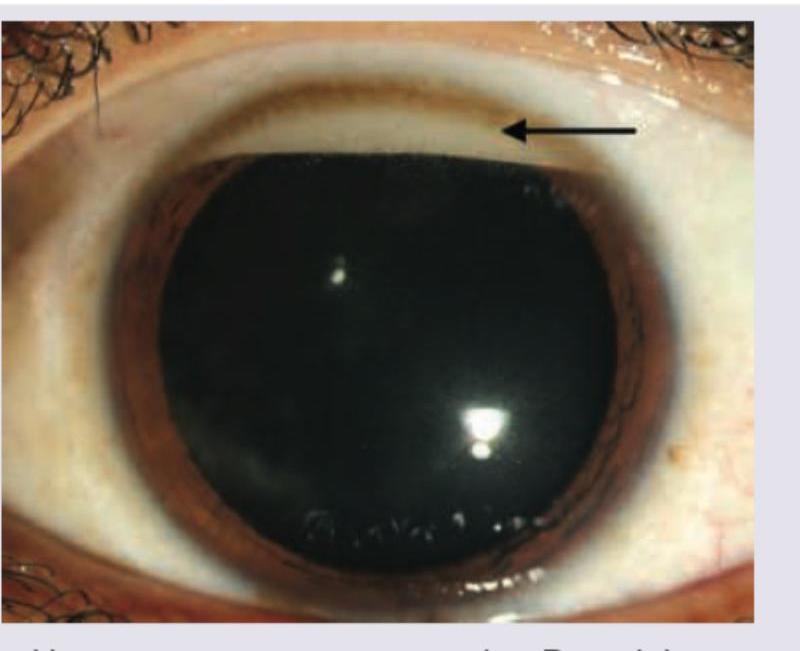
The type of iridectomy shown in the image is:
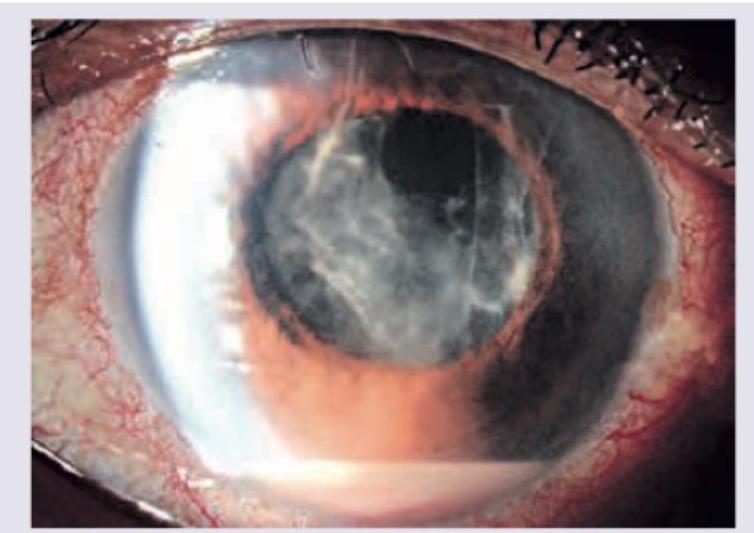
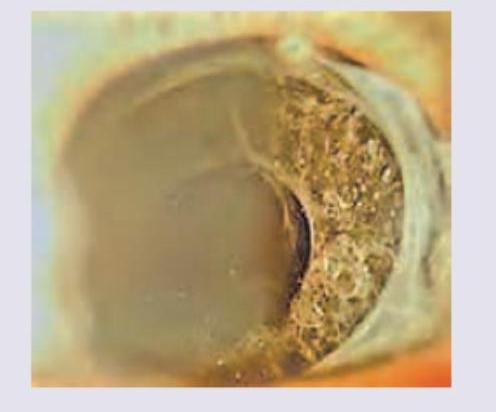
A patient on day 2 after cataract surgery presents with severe eye pain, rapid visual deterioration, poor red reflex, and the following findings which are diagnostic of:
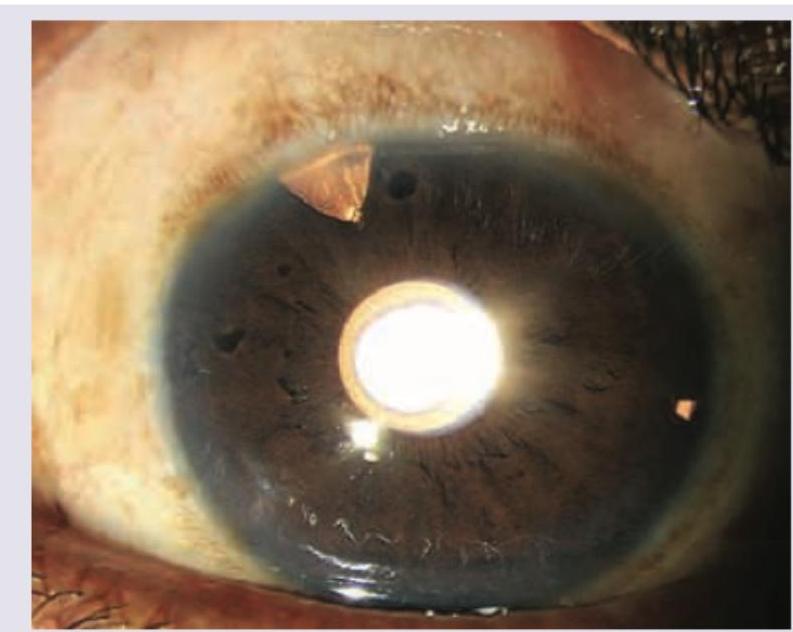
The patient underwent complete iridectomy in aphakia. Comment on the diagnosis:
The image shows an eye following a surgical procedure. What type of iridectomy is depicted?
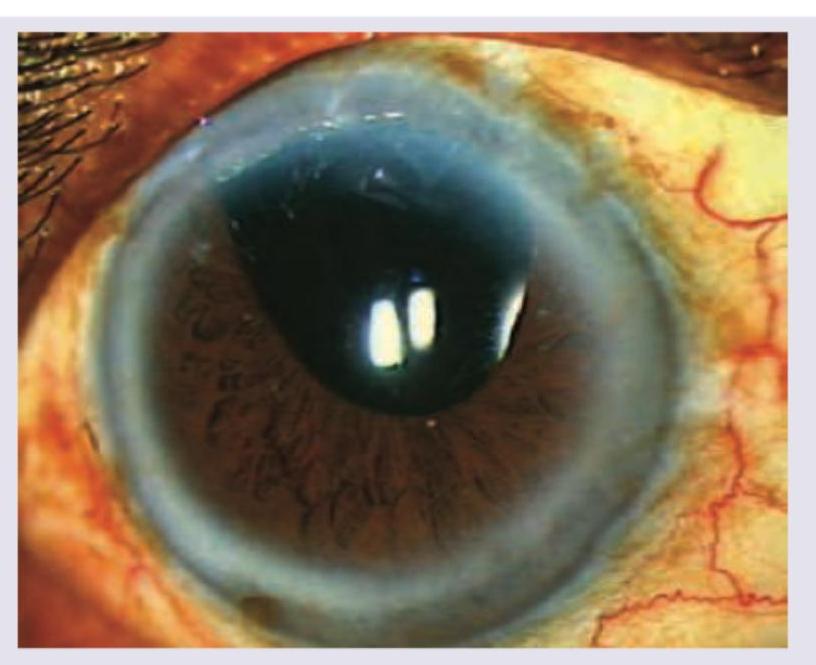
What does the given image show?
A 60-year-old male underwent a cataract surgery. After 1 year he came with complaints of diminished vision and the finding shown in the image. Diagnosis is?
Patient with eye surgery done 2 days ago presents with pain and dimness of vision. Which of the following is not useful for management?
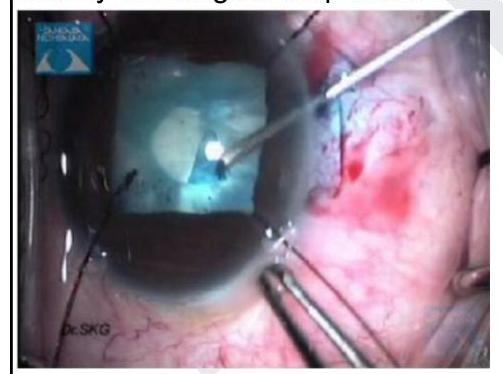
Identify the surgical step shown in the image given below
Evisceration is removal of which layer of eyeball?
Site of bleeding after cataract surgery is:
Practice by Chapter
Surgical Anatomy of Eye
Practice Questions
Asepsis and Sterilization in Eye Surgery
Practice Questions
Anesthesia in Ophthalmic Surgery
Practice Questions
Cataract Surgery Techniques
Practice Questions
Corneal Surgeries
Practice Questions
Glaucoma Surgeries
Practice Questions
Oculoplastic Surgeries
Practice Questions
Vitreoretinal Surgeries
Practice Questions
Strabismus Surgery
Practice Questions
Refractive Surgery
Practice Questions
Ocular Oncology Surgeries
Practice Questions
Management of Surgical Complications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app