
Ophthalmic Surgery — MCQs

On this page
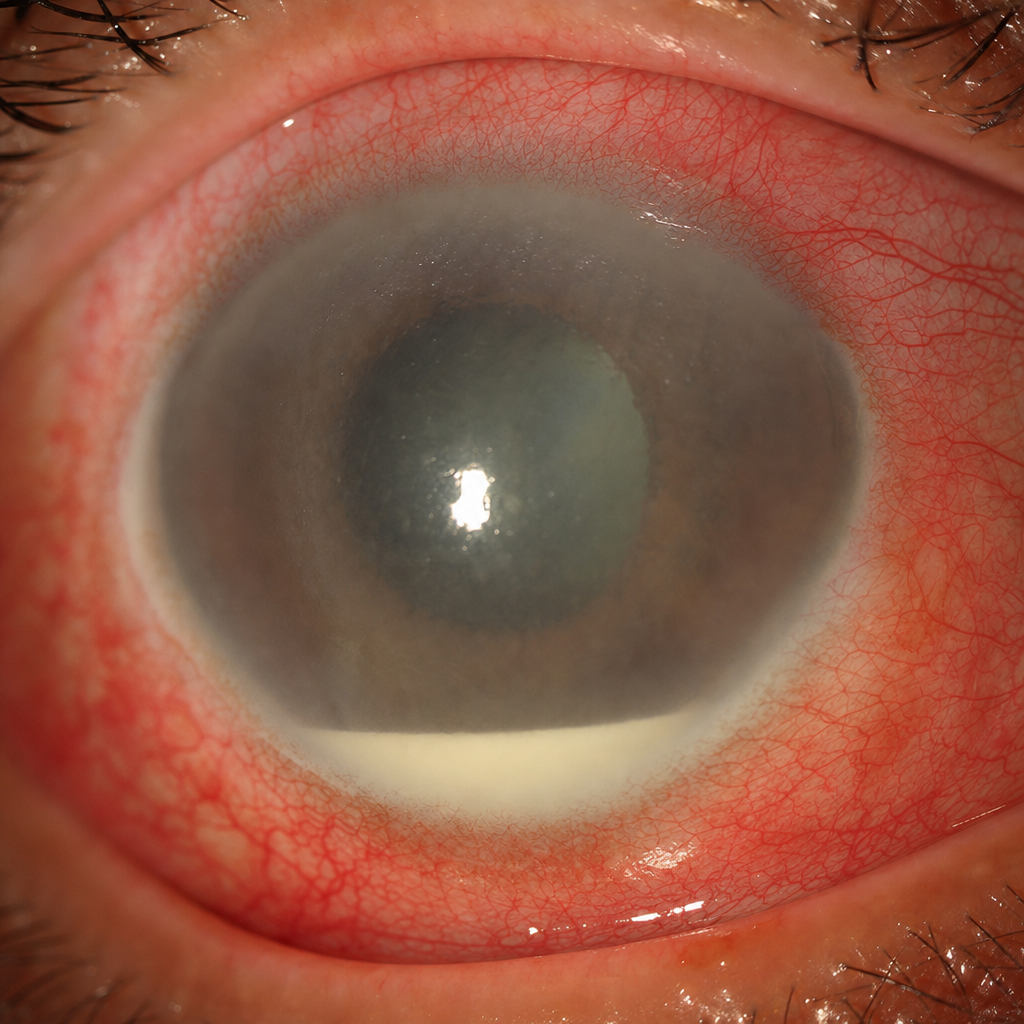
A patient on day 2 after cataract surgery has developed severe pain, marked reduction in vision, vitreous haze, and loss of the red reflex, along with findings seen in the image. These findings are diagnostic of which of the following conditions?
What is the wavelength of the laser used in Femto Laser assisted cataract removal?
Which laser is used for cutting out the cataract capsule?
What is the percentage of endothelial cell loss during Descemet's stripping automated endothelial keratoplasty?
Which of the following is NOT true regarding suprachoroidal hemorrhage?
Which of the following are complications of cataract surgery?
A patient presents with a fixed dilated pupil, iris atrophy, and secondary glaucoma following penetrating keratoplasty. What condition is this suggestive of?
What is the best method to prevent infection after cataract surgery?
Following cataract surgery, a patient comes with complaints of decreased visual acuity. On examination, posterior capsular opacification is seen. What type of laser can be used to treat this condition?
A patient presented 2 weeks after cataract surgery with decreased vision. On examination, there were anterior chamber cells and flare with hazy vitreous. What is the most likely cause and organism?
Practice by Chapter
Surgical Anatomy of Eye
Practice Questions
Asepsis and Sterilization in Eye Surgery
Practice Questions
Anesthesia in Ophthalmic Surgery
Practice Questions
Cataract Surgery Techniques
Practice Questions
Corneal Surgeries
Practice Questions
Glaucoma Surgeries
Practice Questions
Oculoplastic Surgeries
Practice Questions
Vitreoretinal Surgeries
Practice Questions
Strabismus Surgery
Practice Questions
Refractive Surgery
Practice Questions
Ocular Oncology Surgeries
Practice Questions
Management of Surgical Complications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app