
Ophthalmic Surgery — MCQs

On this page
What are the potential complications of a peribulbar block?
Postcataract infection can be prevented by:
What is the ideal fluid for irrigation during Extra Capsular Cataract Extraction (ECCE)?
Recovery in cataract surgery is fastest with which of the following procedures?
Inverse hypopyon is seen in which of the following conditions?
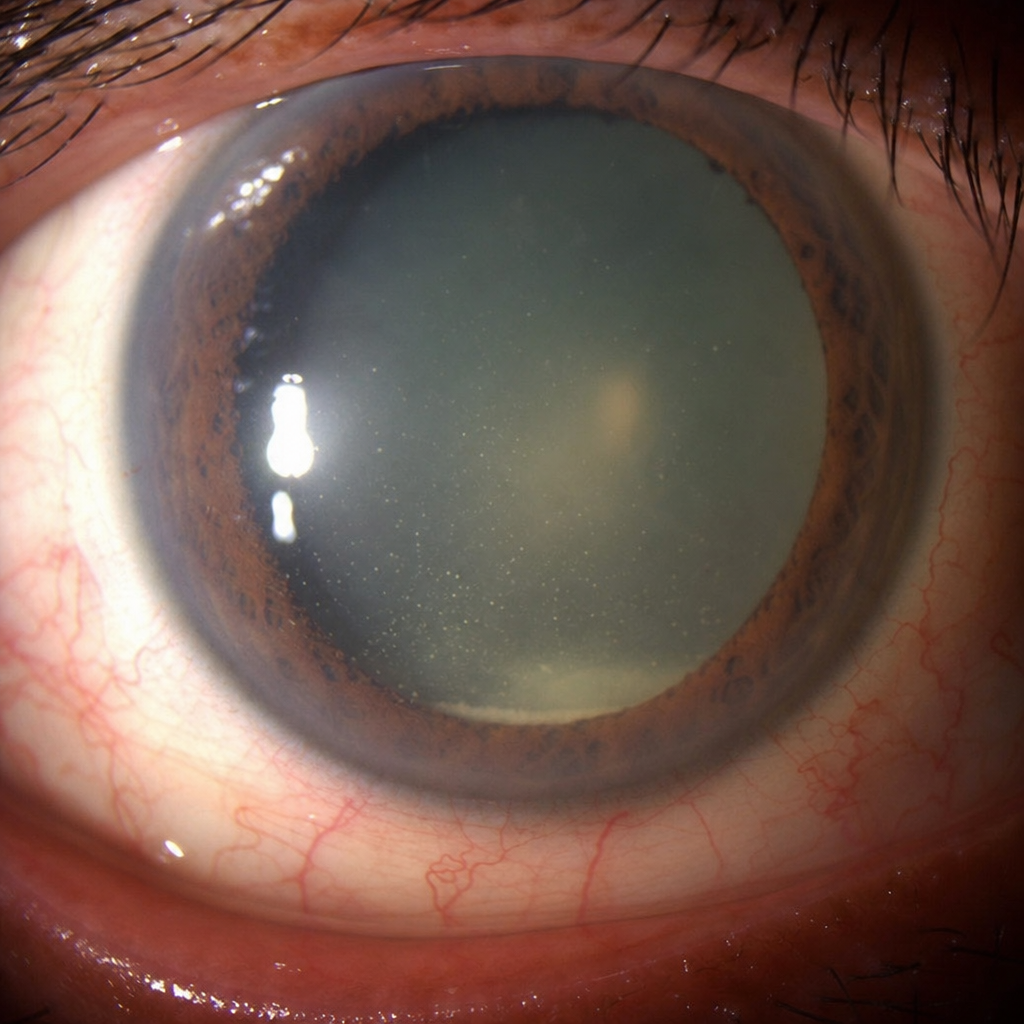
A patient developed pain and severe vision loss 2 days after cataract surgery. On examination, a particular finding was noted. Which of the following statements about the given condition is INCORRECT?
Cystoid macular edema develops commonly after which procedure?
What is the primary power used for nuclear fragmentation in phacoemulsification?
What best describes Extra Capsular Cataract Extraction (ECCE)?
What is the most common complication of extracapsular cataract surgery?
Practice by Chapter
Surgical Anatomy of Eye
Practice Questions
Asepsis and Sterilization in Eye Surgery
Practice Questions
Anesthesia in Ophthalmic Surgery
Practice Questions
Cataract Surgery Techniques
Practice Questions
Corneal Surgeries
Practice Questions
Glaucoma Surgeries
Practice Questions
Oculoplastic Surgeries
Practice Questions
Vitreoretinal Surgeries
Practice Questions
Strabismus Surgery
Practice Questions
Refractive Surgery
Practice Questions
Ocular Oncology Surgeries
Practice Questions
Management of Surgical Complications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app