
Glaucoma Surgeries — MCQs

Argon laser trabeculoplasty is done in:
Uncontrolled hypertension may cause which of the following complications in cataract surgery:
Laser iridotomy is done in?
A crucial step in the phacoemulsification procedure for a 70-year-old man scheduled for cataract surgery is which of the following?
A 56-year-old patient presents after 3 days of cataract surgery with a history of increasing pain and diminished vision after an initial improvement. The most likely cause would be –
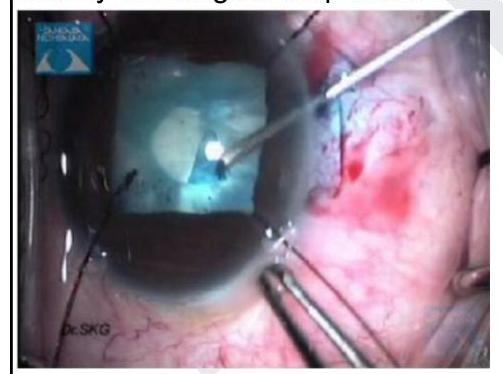
Identify the surgical step shown in the image given below
Expulsive hemorrhage in cataract surgery is from?
In which of the following conditions does IOL implantation after cataract surgery require the greatest caution and specialized management?
What is the preferred surgical technique for traumatic cataract in children?
Which of the following procedures is not typically covered by the National Programme for Control of Blindness (NPCB) for reimbursement of surgery done by a non-governmental organization (NGO) eye hospital?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app