
Anesthesia in Ophthalmic Surgery — MCQs

Premedication is prescribed to – a) Allay anxiety b) Make the patient asleep before coming for operation c) Reduce the dose of induction agents d) Produce amnesia
Which pre-operative investigation is recommended before surgical procedures in a patient on warfarin therapy?
Retrobulbar injection of xylocaine blocks all of the following except:
A patient aged 28 years, was given epidural anesthesia with 15 ml of 1.5% Lignocaine with adrenaline for hernia surgery. He developed hypotension, respiratory arrest and became unconscious within 3 minutes, most probable cause will be:-
Local anaesthetic usually used for retrobulbar block -
What is the maximum dose of plain lignocaine (in mg) for adults?
A 5 year old healthy child is undergoing strabismus surgery with a Laryngeal mask airway in place. Thirty minutes into the procedure, his heart rate is 60 bpm, blood pressure is 90/60 mmHg, and oximeter shows 98% saturation. The next step in management is
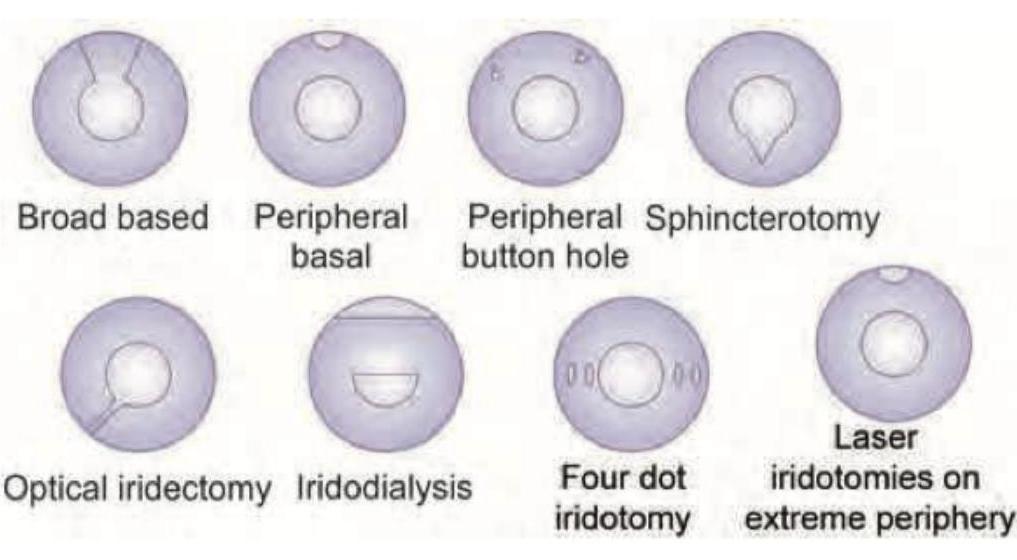
The type of iridectomy shown in the image is:
Which one of the following is a branch of the first part of the maxillary artery?
Identify the ophthalmic instrument used for measuring heterophoria and heterotropia.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app