
Ocular Lubricants — MCQs

Commonest complication of topical corticosteroids is -
Which of the following is Iso-osmolar agent?
Which of the following is a contraindication to topical steroids?
What does the Phenol red thread test assess in relation to dry eye?
In ophthalmology, if a patient is allergic to aminoesters, which local anesthetic can be safely used?
It is essential to lubricate dam before applying it. Which of these is the MOST suitable lubricant?
A young 23-year-old black African man presents with a hyphema in the right eye after blunt injury. All of the following are acceptable initial treatments except?
Distichiasis is a condition characterized by:
Internal hordeolum is due to inflammation of-
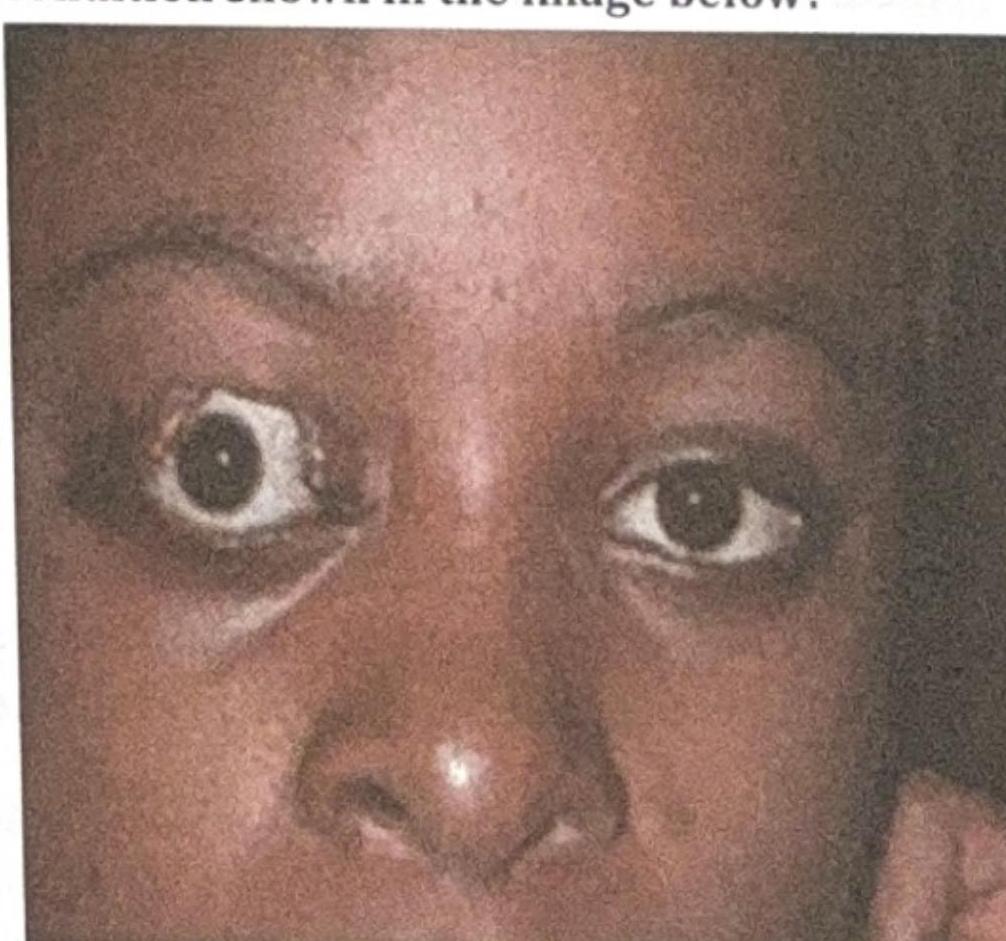
What is the most likely complication of the condition shown in the image below?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app