
Eyelid Anatomy and Physiology — MCQs

10 questions
Read Study NotesQ1
Facial nerve does not supply which structure of the face?
Q2
Unilateral frontal blisters with upper lid edema and conjunctivitis is seen in?
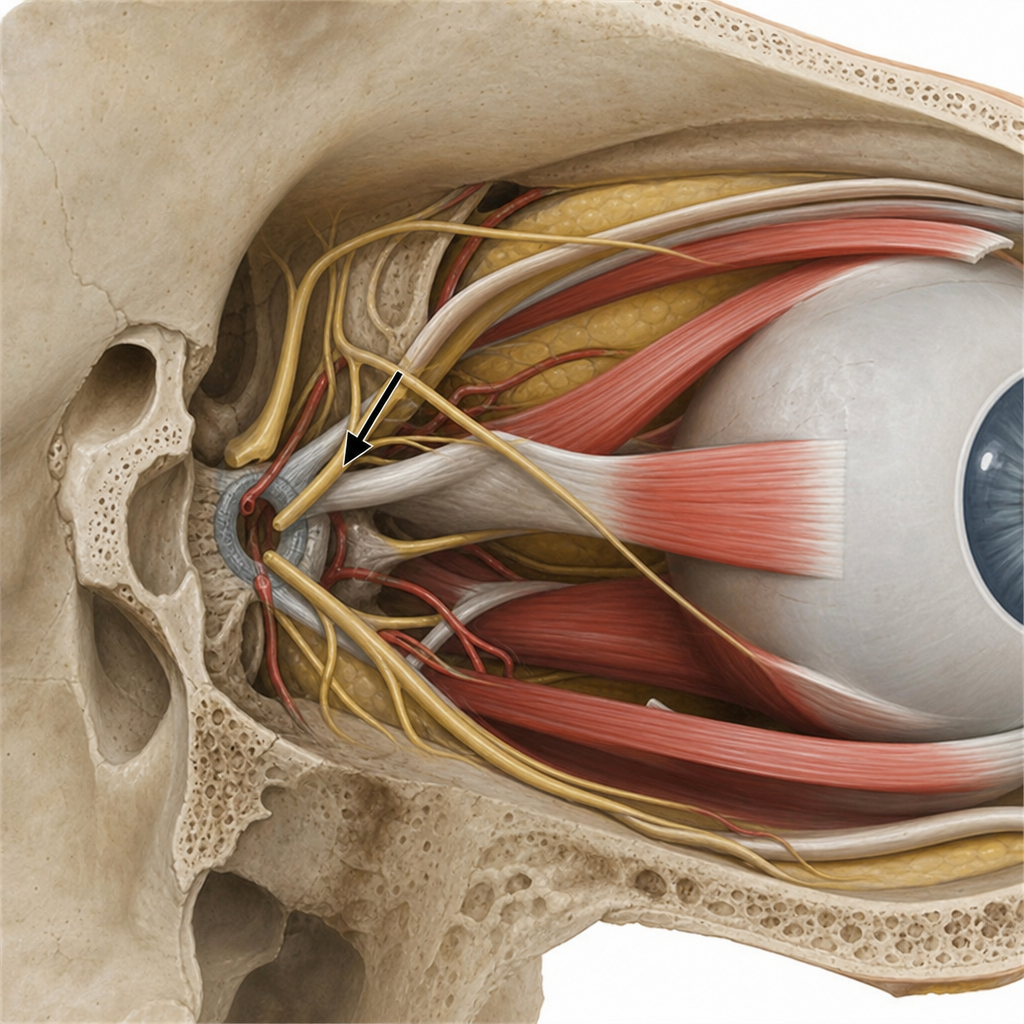
Q3
Lesion of the marked structure affects all EXCEPT
Q4
MC site of basal cell carcinoma of eyelid:
Q5
The infratentorial dura is supplied by branches of the ___?
Q6
Chronic granulomatous inflammation in upper lid (painless swelling) is characteristic of:
Q7
Muscle in the lid attached to posterior tarsal margin is:
Q8
A patient with ptosis has the upper 4 mm of cornea covered by the upper eyelid. What is the grade of ptosis?
Q9
Internal hordeolum is due to inflammation of-
Q10
Distichiasis is a condition characterized by:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app