
Entropion and Ectropion — MCQs

In congenital ptosis, surgery should be performed at the earliest to prevent amblyopia. Which of the following operations is not typically used for the correction of congenital ptosis?
Which of the following is not a type of surgery done for entropion?
What is the term for the fusion of the palpebral and bulbar conjunctiva?
Enophthalmos can be caused by all of the following EXCEPT:
Distichiasis is a condition characterized by:
Fasanella-Servat operation is done for:
Not a feature of ligneous conjunctivitis:
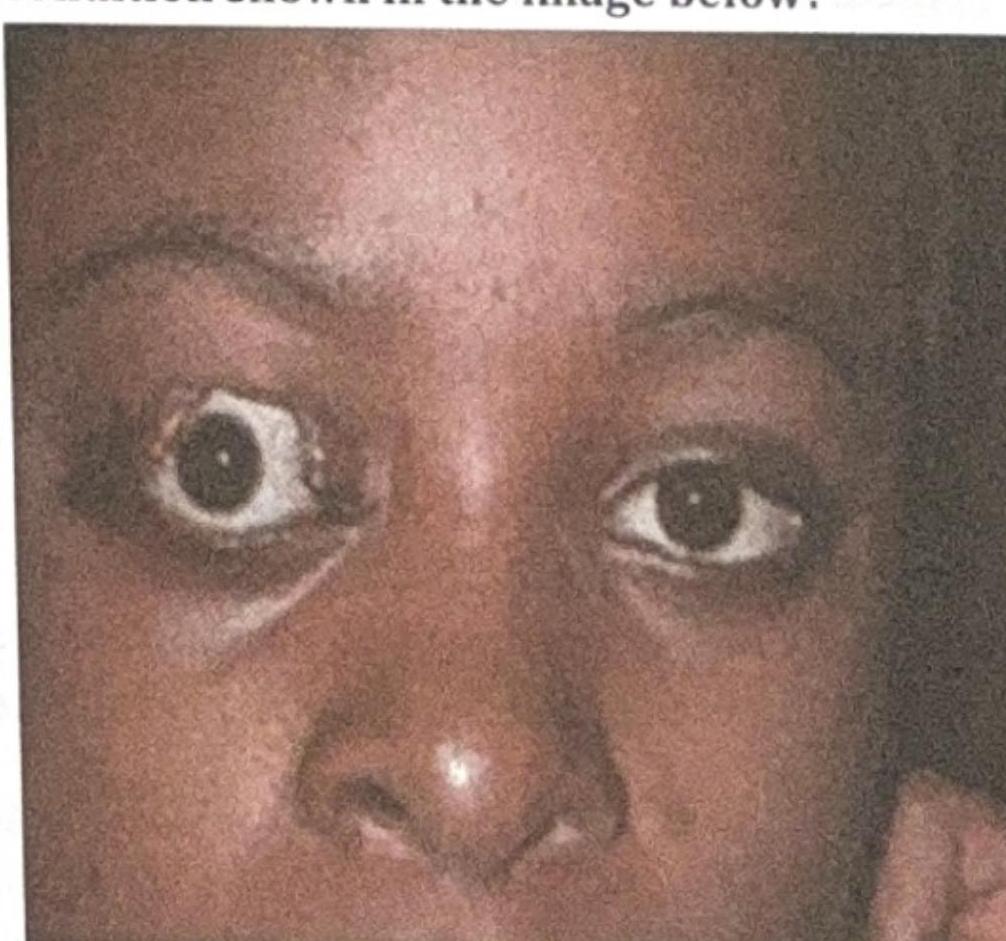
What is the most likely complication of the condition shown in the image below?
Which of the following intraocular foreign bodies causes severe toxicity and needs to be removed promptly?
Identify the lesion.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app