
Ocular Trauma — MCQs

On this page
A patient has a history of a flying metallic foreign body injury to the eye. On examination, there is evidence of intraocular metallic foreign body with progressive visual deterioration. Which of the following substances is most likely causing the toxic deposition in ocular tissues?
A patient sustained blunt trauma to the eye 6 months ago and now presents with blurring of vision. What is the most likely condition?
A patient presents to you with pain and redness in the right eye following an injury during welding. On examination, visual acuity is preserved, slit-lamp examination confirms the foreign body is superficial, the Seidel test is negative, and there are no signs of an intraocular foreign body. The following is also observed. Which of the following is the appropriate next step in managing this patient? 
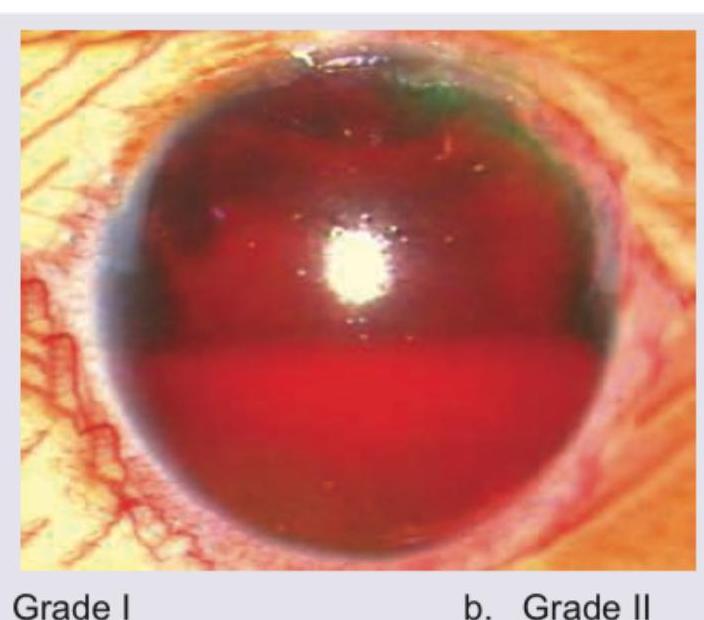
Which of the following is correct about the image shown below?

Comment on the grade of the lesion shown in the image.
Blow out fracture can be due to:
Perforating injuries with retained intraocular foreign body are more serious than those without because of:
Sympathetic ophthalmia is due to
A patient sustained blunt trauma to the eye, after which he developed sudden loss of vision with deep anterior chamber. Most likely cause is:
In a patient with a metallic foreign body in the eye, which investigation should NOT be done?
Practice by Chapter
Classification of Ocular Trauma
Practice Questions
Blunt Trauma
Practice Questions
Penetrating and Perforating Injuries
Practice Questions
Intraocular Foreign Bodies
Practice Questions
Chemical Injuries
Practice Questions
Thermal and Radiation Injuries
Practice Questions
Orbital Trauma
Practice Questions
Traumatic Optic Neuropathy
Practice Questions
Ocular Manifestations of Child Abuse
Practice Questions
Sports-Related Eye Injuries
Practice Questions
Ocular Trauma Management Principles
Practice Questions
Rehabilitation After Ocular Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app