
Intraocular Foreign Bodies — MCQs

Kayser-Fleischer rings (KF rings) are seen in:
A patient presents with acute appendicitis. What is NOT to be done?
Which of the following intraocular foreign bodies causes severe toxicity and needs to be removed promptly?
Perforating injuries with retained intraocular foreign body are more serious than those without because of:
Best method of detection of a retained glass intraocular foreign body is
In a patient with a metallic foreign body in the eye, which investigation should NOT be done?
A laborer working in a construction site has a history of chuna particles falling in eye. Next step of management is
Best method of detection of retained glass intraocular foreign body is:
Which of the following ophthalmologic conditions shows 'Vossius ring' during examination?
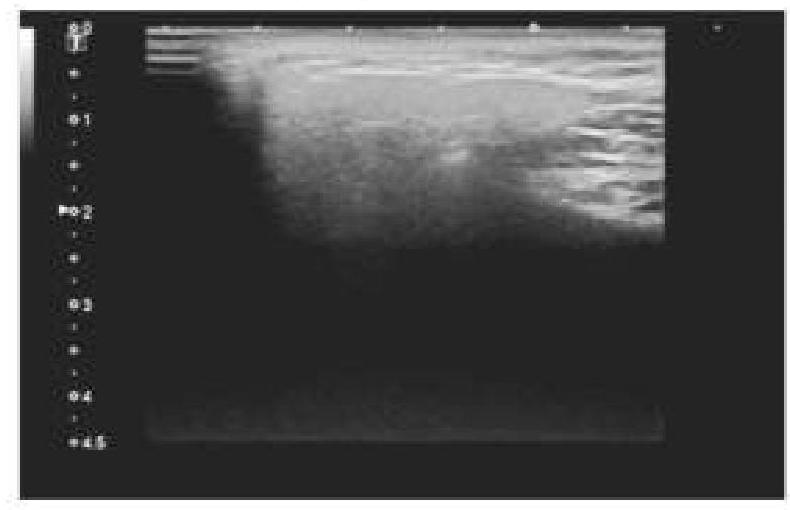
A 45-year-old patient complained of pain on one side of the neck. She is afraid of eating food as it worsens the pain. An ultrasound of the salivary glands is shown below. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app