
Ocular Manifestations of Systemic Disorders — MCQs

On this page
A Dalen-Fuchs lesion is typically seen in which of the following conditions?
Lisch nodule is seen in which of the following conditions?
A 2-year-old unimmunized child from a hilly tribal area developed Keratomalacia after a viral infection. Which of the following viral infections could have led to the development of Keratomalacia?
Which condition presents with uveitis, auditory problems, and cutaneous issues?
What is the most common intraocular tumor in adults?
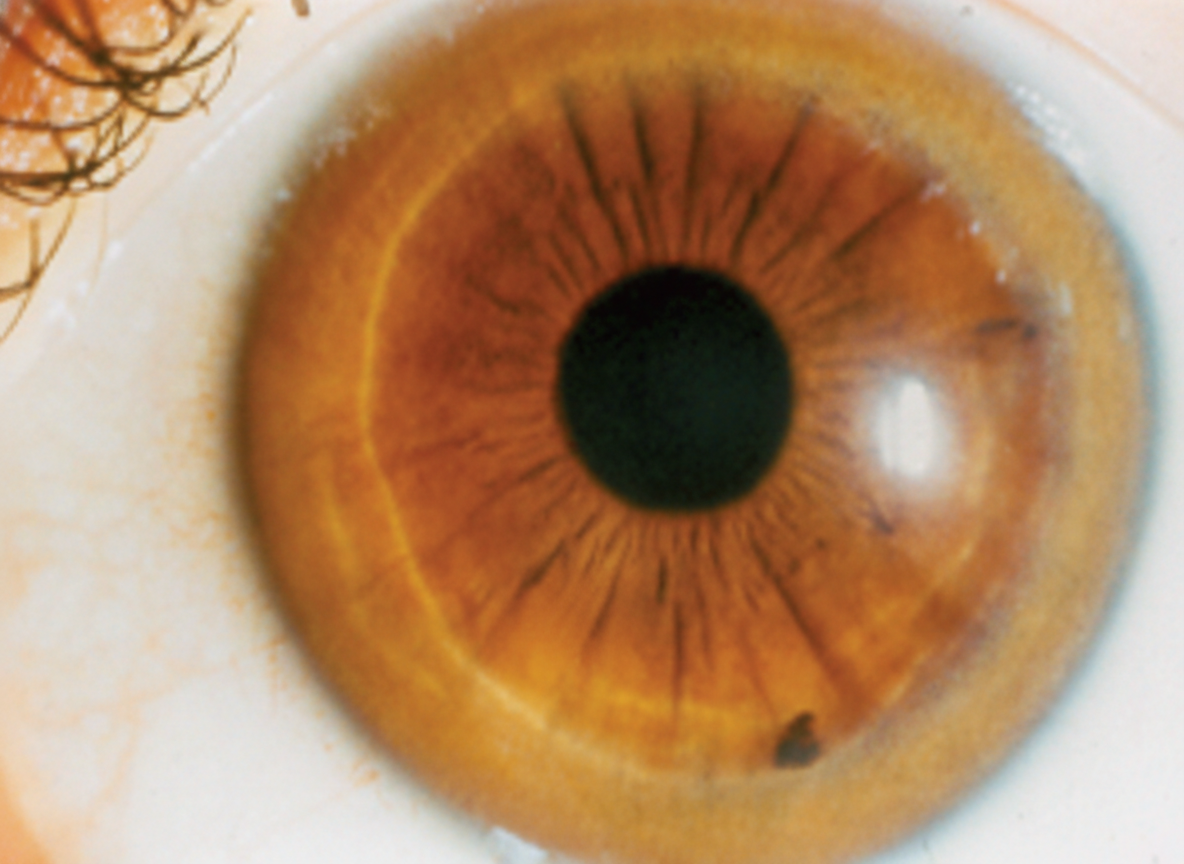
A 10-year-old child presents with Fanconi's syndrome. Which of the following ocular findings is most characteristic?
Systemic corticosteroids in herpes zoster ophthalmicus are indicated when associated with which of the following conditions?
Red keratin precipitates are seen in which of the following conditions?
Diagnose the condition.
The use of highly active anti-retroviral therapy (HAART) is associated with the development of:
Practice by Chapter
Diabetes Mellitus
Practice Questions
Hypertension
Practice Questions
Autoimmune Disorders
Practice Questions
Thyroid Disease
Practice Questions
HIV and AIDS
Practice Questions
Hematological Disorders
Practice Questions
Neurological Disorders
Practice Questions
Dermatological Conditions
Practice Questions
Pregnancy-Related Eye Changes
Practice Questions
Metabolic Disorders
Practice Questions
Ocular Toxicity of Systemic Medications
Practice Questions
Infectious Systemic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app