
Ocular Manifestations of Systemic Disorders — MCQs

On this page
River blindness is caused by which of the following?
Essential atrophy of the choroid is due to an inborn error of metabolism of which amino acid?
All of the following are ocular symptoms seen in Herpes ophthalmicus, EXCEPT:
Uveitis is most commonly associated with which condition?
What condition is characterized by "candle-wax spots" in the retina?
Conjunctival xerosis is caused by which vitamin deficiency?
Optic nerve glioma is seen in?
Which vitamin deficiency causes xerophthalmia, a condition which causes dry eyes?
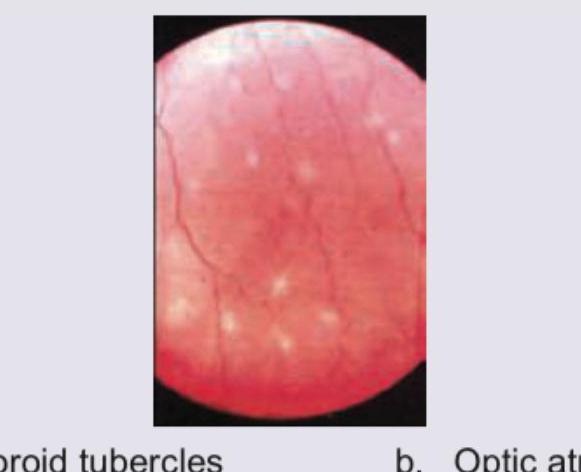
What does the fundus of this immunocompromised patient show?
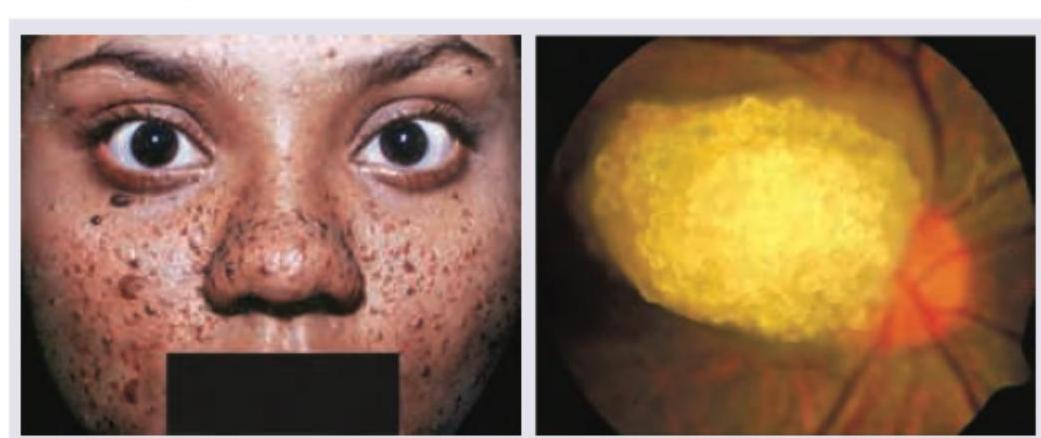
A 16-year-old girl with history of epilepsy has the presentation as shown below. Select the correct option:
Practice by Chapter
Diabetes Mellitus
Practice Questions
Hypertension
Practice Questions
Autoimmune Disorders
Practice Questions
Thyroid Disease
Practice Questions
HIV and AIDS
Practice Questions
Hematological Disorders
Practice Questions
Neurological Disorders
Practice Questions
Dermatological Conditions
Practice Questions
Pregnancy-Related Eye Changes
Practice Questions
Metabolic Disorders
Practice Questions
Ocular Toxicity of Systemic Medications
Practice Questions
Infectious Systemic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app