
Ocular Manifestations of Systemic Disorders — MCQs

On this page
Copper deposition in the cornea leads to what finding?
What is Hutchinson's rule in relation to herpes zoster ophthalmicus?
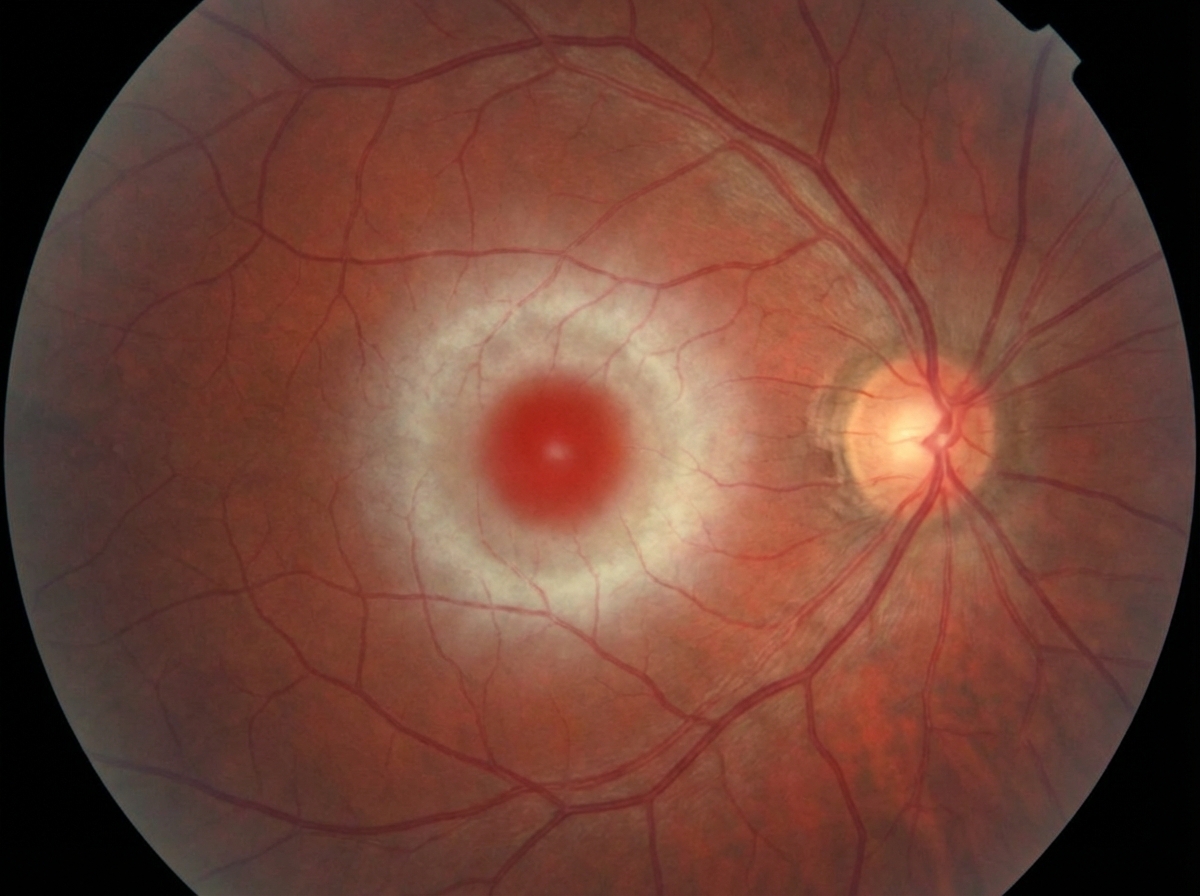
In which of the following diseases is the eye finding shown below seen?
Roth spots are commonly seen in:
What is the most common complication of acute anterior uveitis?
A positive fluorescein dye disappearance test indicates that watering of the eye is due to which of the following?
What is the typical pupil appearance in an acute anterior uveitis attack?
Mutton fat keratic precipitate and Busacca nodules are seen in which type of uveitis?
What is the commonest infection causing blindness in adult men?
A patient presents with freckling in the axilla and inguinal area since childhood. Which of the following is NOT an ophthalmological examination finding in such a patient?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Hypertension
Practice Questions
Autoimmune Disorders
Practice Questions
Thyroid Disease
Practice Questions
HIV and AIDS
Practice Questions
Hematological Disorders
Practice Questions
Neurological Disorders
Practice Questions
Dermatological Conditions
Practice Questions
Pregnancy-Related Eye Changes
Practice Questions
Metabolic Disorders
Practice Questions
Ocular Toxicity of Systemic Medications
Practice Questions
Infectious Systemic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app