
Ocular Manifestations of Systemic Disorders — MCQs

On this page
What is the most common ocular involvement in sarcoidosis?
In retinoblastoma, after enucleation, which tissue is sectioned to determine the extent of spread?
Which ocular structure is commonly involved in sympathetic ophthalmia?
What ocular structures are involved in Staphylococcal blepharitis?
Sympathetic ophthalmia is defined as:
Vitamin A deficiency is characterized by all EXCEPT:
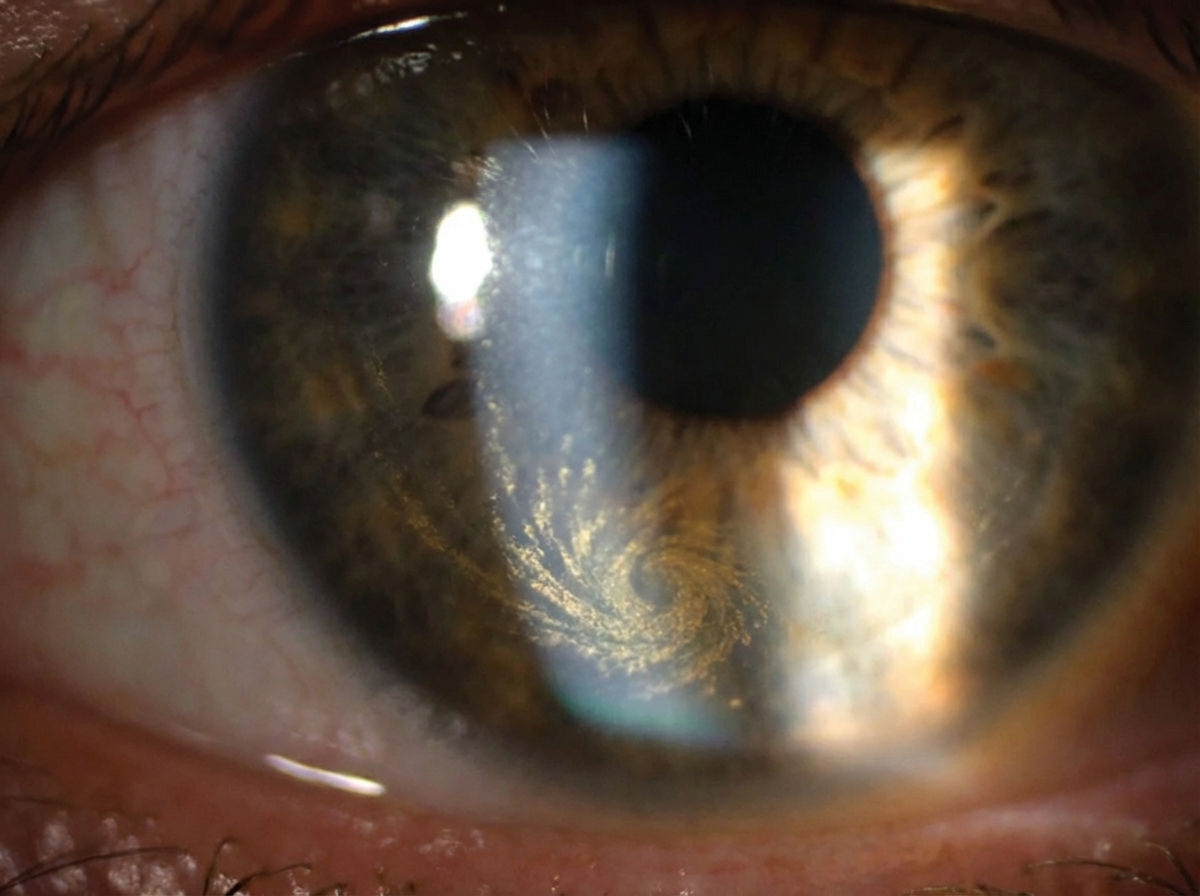
A 55-year-old cardiac patient on long-term treatment presents for a follow-up visit. The physician observes a specific finding on ophthalmological examination. Which drug prescribed by the physician is most likely responsible for this finding?
A patient presents to the eye outpatient department with recurrent chalazion. Which of the following types of cancer should be excluded in these patients?
What is the most common ophthalmological manifestation of the X-linked form of Alport syndrome?
Ocular manifestations of vitamin D deficiency include:
Practice by Chapter
Diabetes Mellitus
Practice Questions
Hypertension
Practice Questions
Autoimmune Disorders
Practice Questions
Thyroid Disease
Practice Questions
HIV and AIDS
Practice Questions
Hematological Disorders
Practice Questions
Neurological Disorders
Practice Questions
Dermatological Conditions
Practice Questions
Pregnancy-Related Eye Changes
Practice Questions
Metabolic Disorders
Practice Questions
Ocular Toxicity of Systemic Medications
Practice Questions
Infectious Systemic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app