
Ocular Manifestations of Systemic Disorders — MCQs

On this page
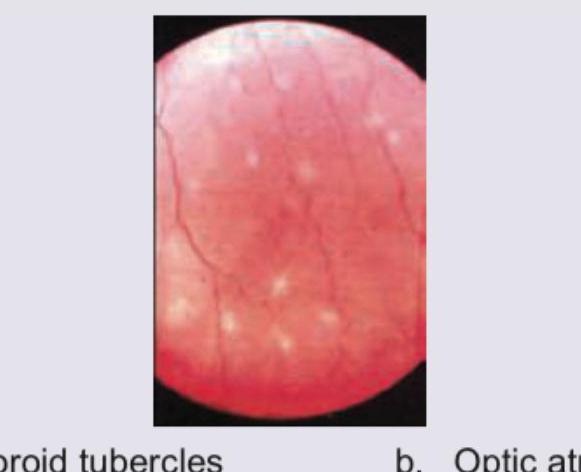
What does the fundus of this immunocompromised patient show?
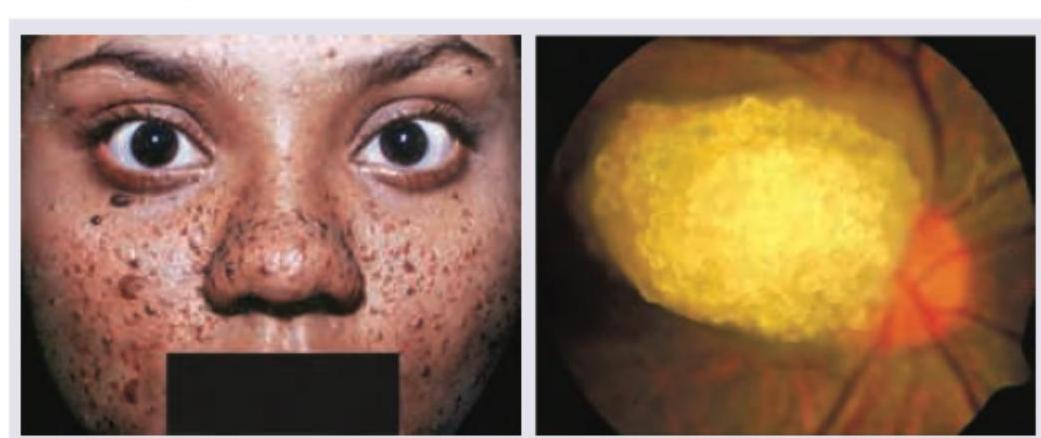
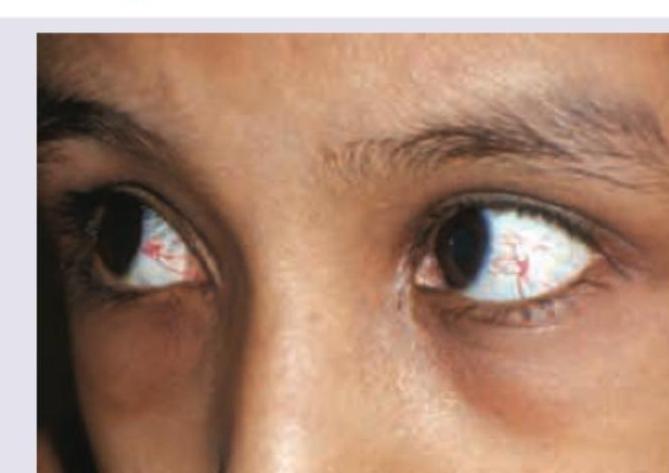
A 16-year-old girl with history of epilepsy has the presentation as shown below. Select the correct option:
A 30-year-old school teacher presents with complaints of red eye with photophobia. Ocular findings are shown below. All are true about the condition shown except: (Recent NEET Pattern 2016-17)
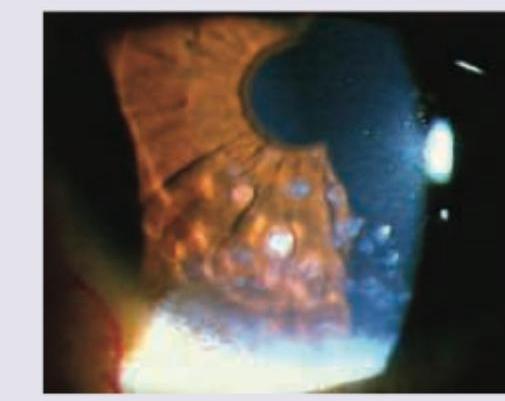
A patient presents with the clinical findings shown in the image. What is the most likely diagnosis?

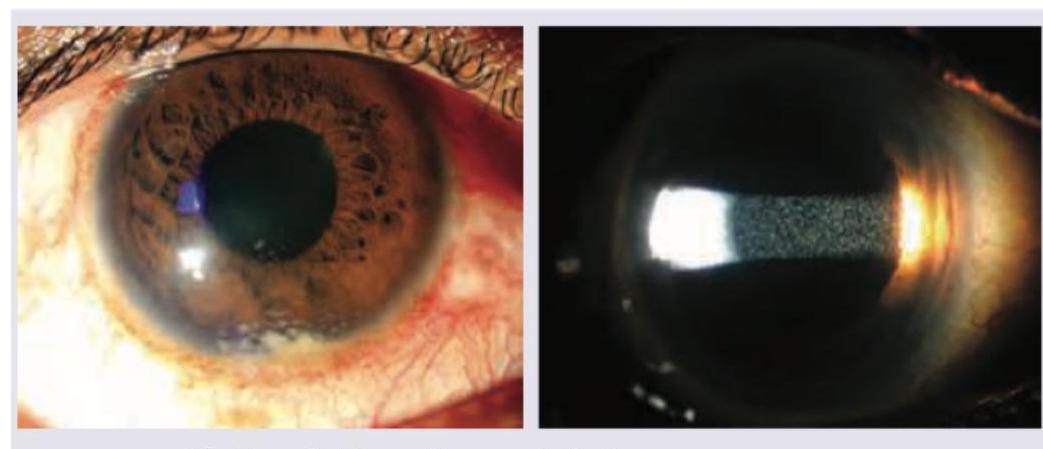
A 15-year-old child was diagnosed with Fanconi's syndrome. His school grades have been consistently poor and he has involuntary movements in his hands. Drug screening is negative. Eye finding shows: (APPG 2016)

What does the following image show?
The image shows a child with?
Of the following ocular manifestations of Vitamin A deficiency, the first sign that can be clinically seen is:
The most common ocular lesion peculiar to HIV infection in early stage is :
In patients with systemic hypertension, the characteristic haemorrhage seen on ophthalmoscopy is
Practice by Chapter
Diabetes Mellitus
Practice Questions
Hypertension
Practice Questions
Autoimmune Disorders
Practice Questions
Thyroid Disease
Practice Questions
HIV and AIDS
Practice Questions
Hematological Disorders
Practice Questions
Neurological Disorders
Practice Questions
Dermatological Conditions
Practice Questions
Pregnancy-Related Eye Changes
Practice Questions
Metabolic Disorders
Practice Questions
Ocular Toxicity of Systemic Medications
Practice Questions
Infectious Systemic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app