
Ocular Manifestations of Systemic Disorders — MCQs

On this page
Anterior uveitis is characterized by which of the following?
Which of the following is NOT a feature of Behcet's disease?
Which of the following metabolic disorders is associated with the fundoscopic finding shown in the image?

A 68-year-old woman with a history of left ventricular congestive heart failure has had decreased visual acuity for the past 5 years. She has no ocular pain and her intraocular pressure is normal. Funduscopic examination reveals arteriolar narrowing, flame-shaped hemorrhages, cotton-wool spots, and hard, waxy exudates. Which of the following underlying diseases is she most likely to have?
What is the most common ocular manifestation in rheumatoid arthritis?
Significant loss of vision in a patient with hypertension can occur due to all of the following, except?
Bilateral skin depigmentation, chronic uveitis, and tinnitus are features of which syndrome?
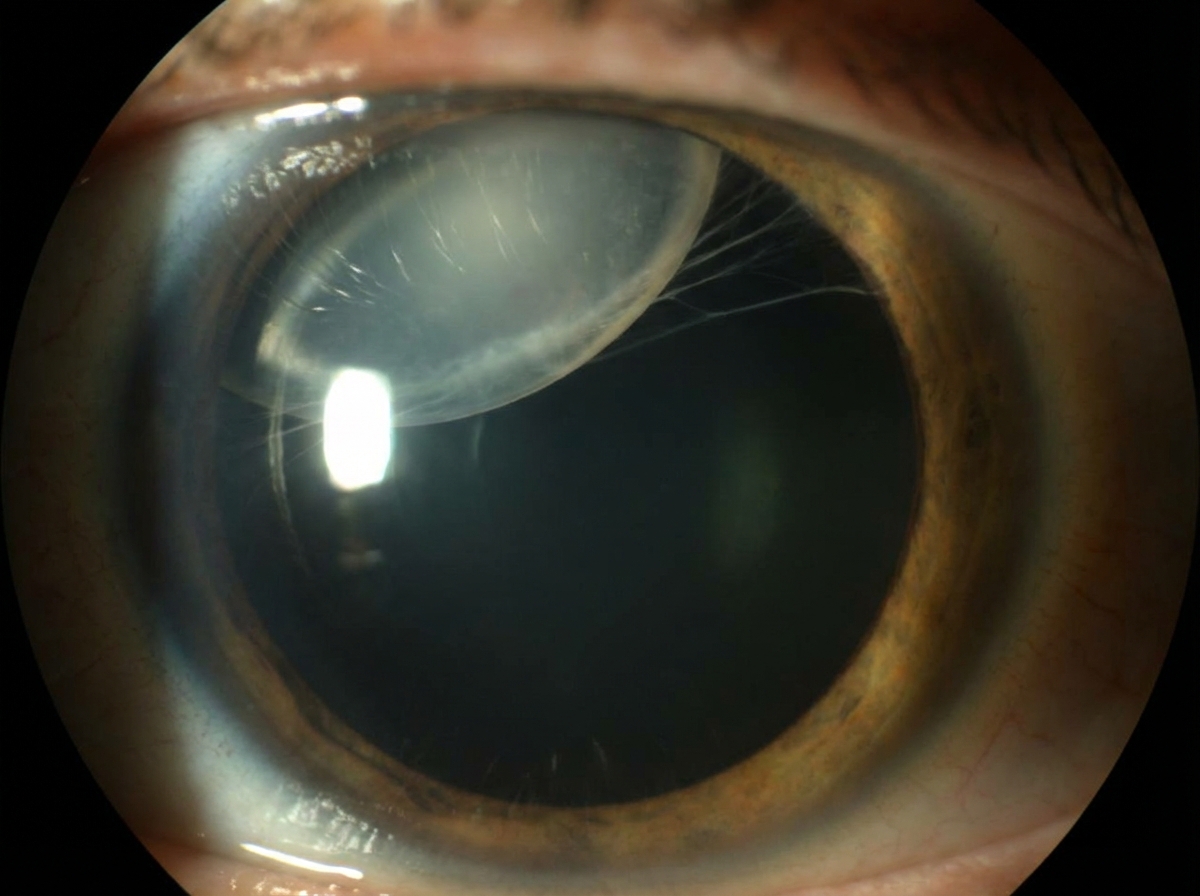
What is the diagnosis in this 31-year-old tall woman with gradual bilateral vision loss, long fingers, and a history of aortic root dilatation?
Which of the following is NOT an ophthalmic finding of acute meningococcal meningitis?
Which of the following is true about heterochromic uveitis?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Hypertension
Practice Questions
Autoimmune Disorders
Practice Questions
Thyroid Disease
Practice Questions
HIV and AIDS
Practice Questions
Hematological Disorders
Practice Questions
Neurological Disorders
Practice Questions
Dermatological Conditions
Practice Questions
Pregnancy-Related Eye Changes
Practice Questions
Metabolic Disorders
Practice Questions
Ocular Toxicity of Systemic Medications
Practice Questions
Infectious Systemic Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app