
Neuro-Ophthalmology — MCQs

On this page
Which of the following is TRUE regarding conical blindness?
A 40-year-old female presented with an excruciating headache, ptosis, downward and outward gaze of the eyeball, and a large pupil. She also complained of blurred and double vision. An magnetic resonance angiogram scan showed an aneurysm of the circle of Willis. Which artery gives rise to the offending aneurysm?
The swinging flashlight test is used to examine which part of the eye?
The use of highly active anti-retroviral therapy (HAART) is associated with the development of which of the following ocular conditions?
In the normal human right eye, the peripheral field of vision is usually least in which direction?
Papilledema is caused by tumors arising from all the following structures except:
Anisocoria in dim light is maximally seen in which condition?
All of the following findings are associated with optic neuritis except?
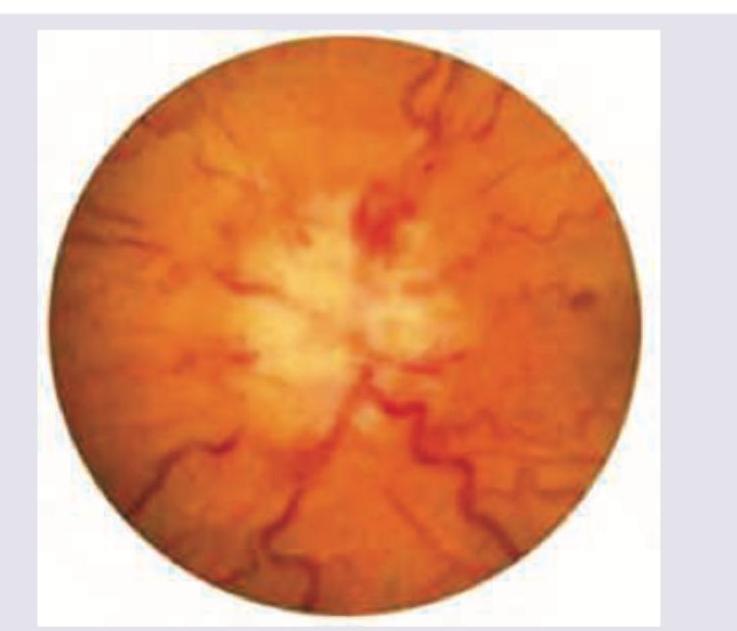
Diagnose the ocular pathology.
Which of the following is NOT a psychogenic complaint related to vision?
Practice by Chapter
Anatomy of Visual Pathways
Practice Questions
Pupillary Disorders
Practice Questions
Optic Neuritis
Practice Questions
Ischemic Optic Neuropathies
Practice Questions
Other Optic Neuropathies
Practice Questions
Papilledema
Practice Questions
Cranial Nerve Palsies
Practice Questions
Nystagmus
Practice Questions
Visual Field Defects
Practice Questions
Neuro-ophthalmic Manifestations of Intracranial Lesions
Practice Questions
Functional Visual Disorders
Practice Questions
Migraine and the Eye
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app