
Neuro-Ophthalmology — MCQs

On this page
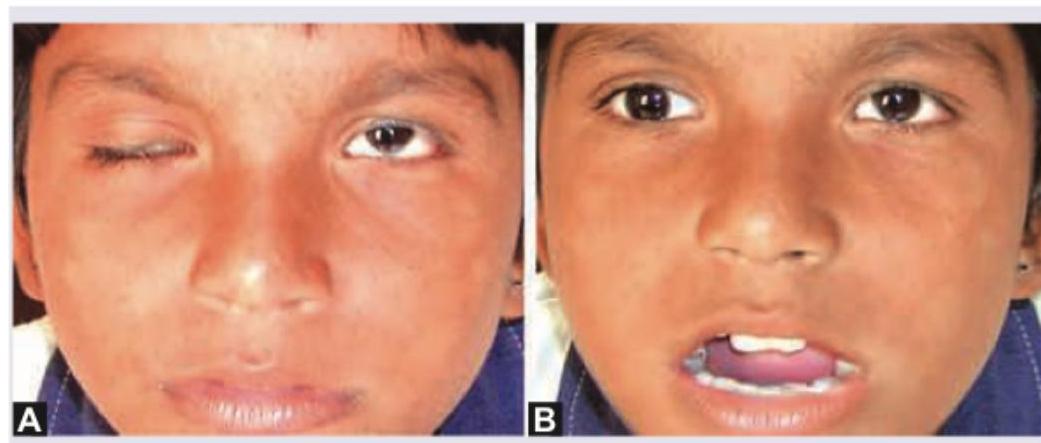
A 10-year-old girl child presents with ptosis of right eyelid. On movement of jaw there is retraction of ptotic eyelid. The image of the patient is shown below. This condition is known as:
An 8-year-old child presents with gradual reduction in vision in the right eye. Family history of similar presentation was elicited on the maternal side. On examination, on right side direct light reflex is absent and consensual light reflex is present. Fundus examination was performed. What is the diagnosis?

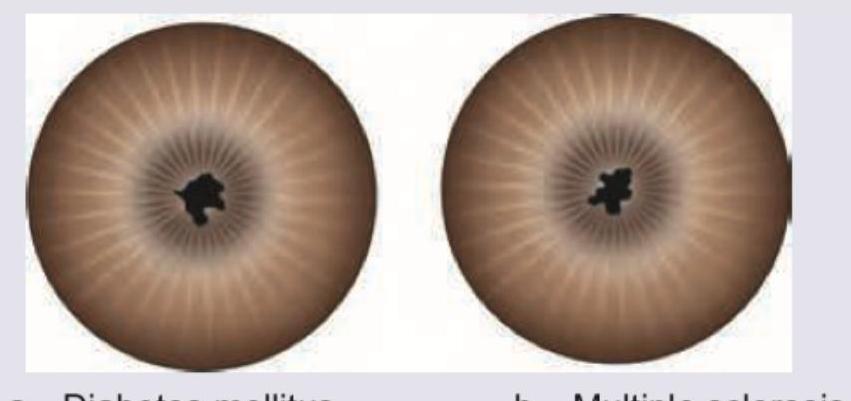
The pupils shown below are miotic and irregular in shape. They are nonreactive to light but react to accommodation. They also do not dilate with atropine. All are causes of these pupils except:
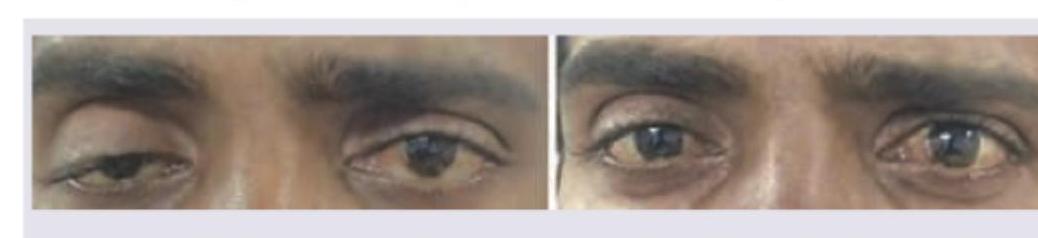
A 25-year-old lady presents with reduced color vision and paresthesias. Her symptoms increase with rise of body temperature. Examine the appearance of her eyes and comment on diagnosis.

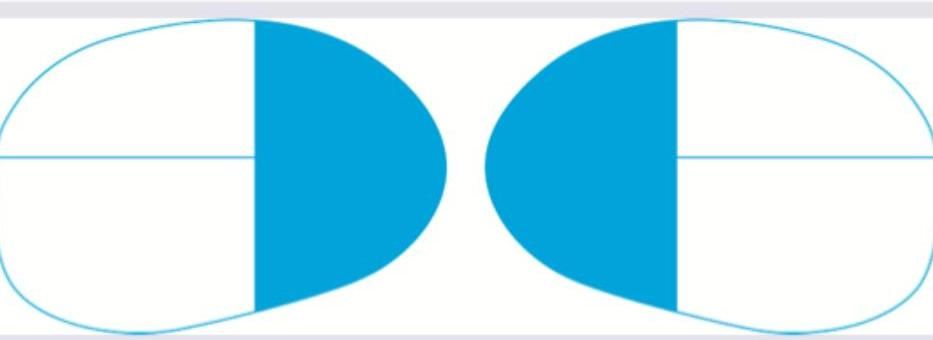
The following visual loss is seen due to lesion in:
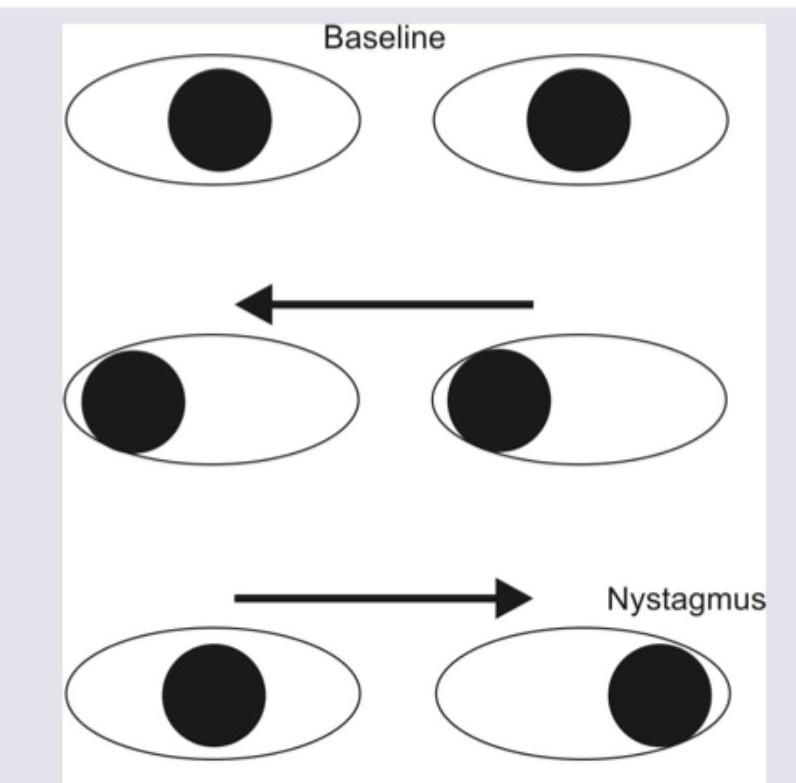
A patient presents with the eye movement abnormalities shown in the image below. What is the diagnosis?
What is the diagnosis?
The given image shows which of the following conditions? (AIIMS Nov 2018)

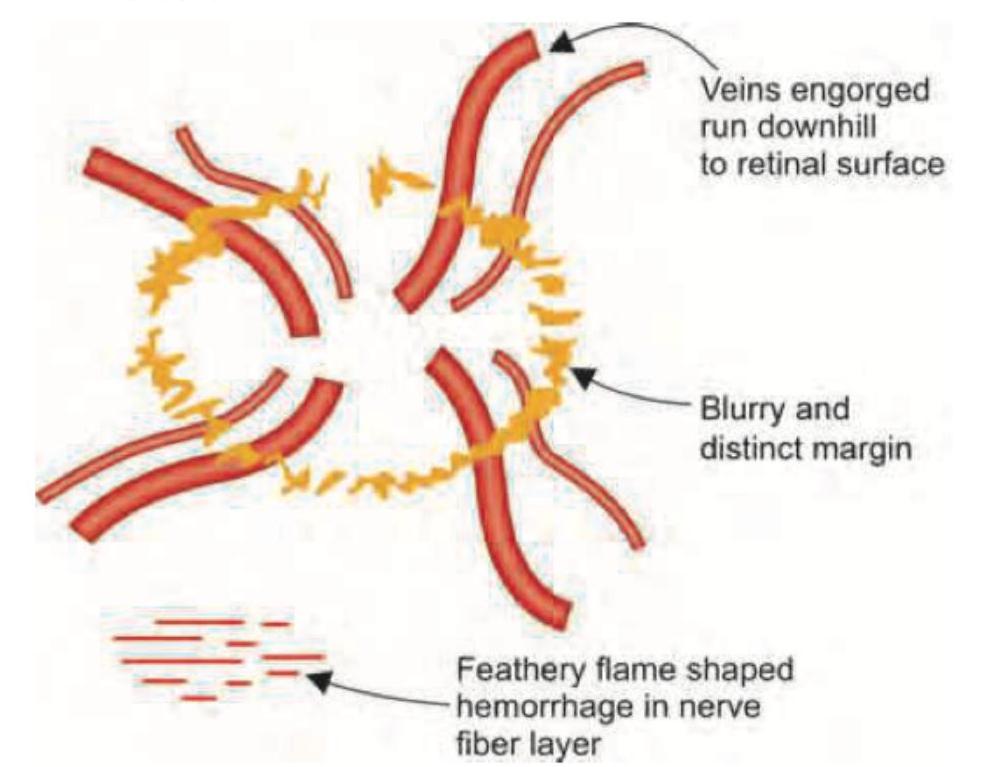
The images show a normal optic disc (left) and papilledema with blurred disc margins (right). What is the most common cause of this condition?
Identify the visual field defect shown in the image.

Practice by Chapter
Anatomy of Visual Pathways
Practice Questions
Pupillary Disorders
Practice Questions
Optic Neuritis
Practice Questions
Ischemic Optic Neuropathies
Practice Questions
Other Optic Neuropathies
Practice Questions
Papilledema
Practice Questions
Cranial Nerve Palsies
Practice Questions
Nystagmus
Practice Questions
Visual Field Defects
Practice Questions
Neuro-ophthalmic Manifestations of Intracranial Lesions
Practice Questions
Functional Visual Disorders
Practice Questions
Migraine and the Eye
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app