
Neuro-Ophthalmology — MCQs

On this page
What is the first sign of optic nerve disease?
Which of the following is associated with an altitudinal visual field defect?
What is the best investigation for optic neuritis?
Bitemporal hemianopia is typically seen in which of the following conditions?
A patient presents with diplopia, headache, and blurring of vision. On examination, while attempting to gaze to the right, the right eye abducts but the left eye fails to adduct. The patient's rightward gaze is normal, and convergence is also normal. Where is the lesion most likely located?
Which of the following is NOT a feature of Horner's syndrome?
Which of the following conditions can result in bitemporal hemianopia?
Disc oedema is seen in which of the following conditions?
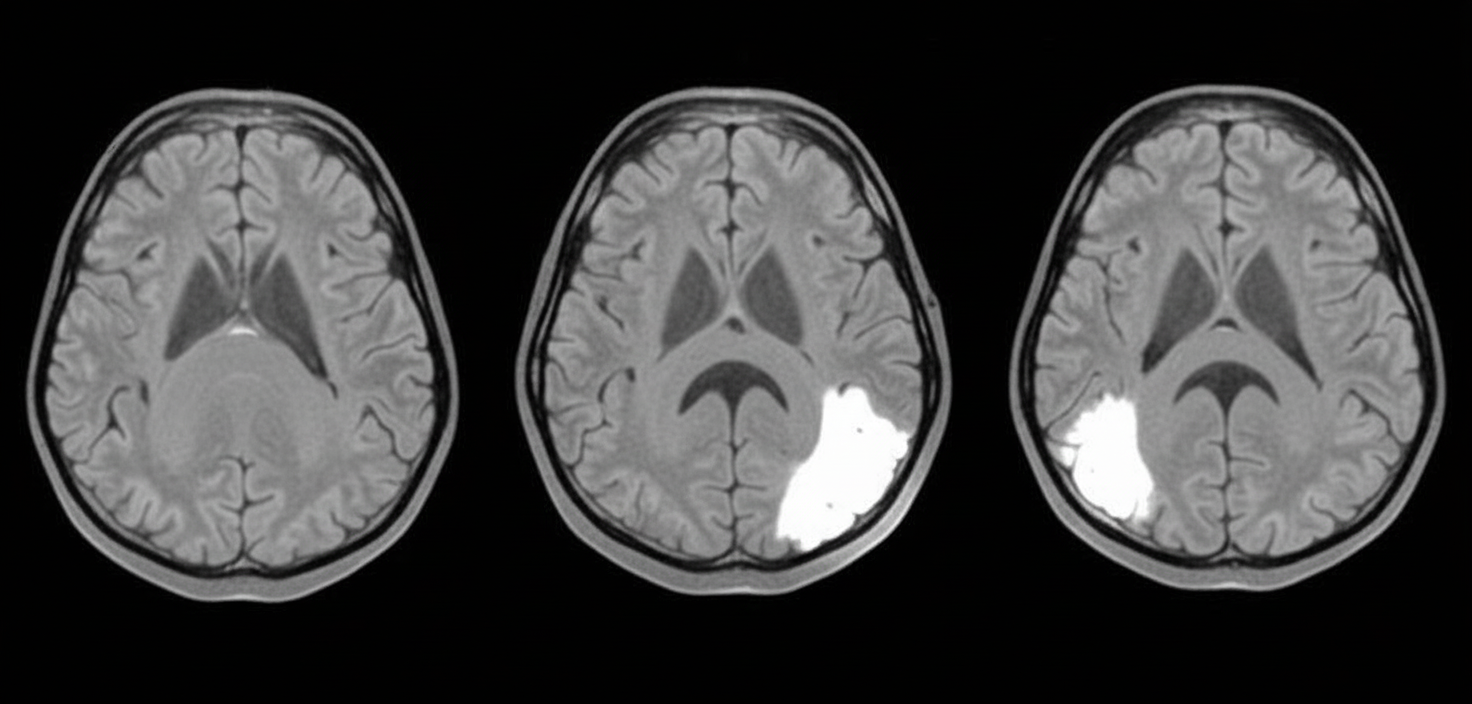
Which one of the following patterns of visual disturbance would be demonstrable on examination of this patient?
Papilloedema is characterised by all of the following, EXCEPT:
Practice by Chapter
Anatomy of Visual Pathways
Practice Questions
Pupillary Disorders
Practice Questions
Optic Neuritis
Practice Questions
Ischemic Optic Neuropathies
Practice Questions
Other Optic Neuropathies
Practice Questions
Papilledema
Practice Questions
Cranial Nerve Palsies
Practice Questions
Nystagmus
Practice Questions
Visual Field Defects
Practice Questions
Neuro-ophthalmic Manifestations of Intracranial Lesions
Practice Questions
Functional Visual Disorders
Practice Questions
Migraine and the Eye
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app