
Neuro-Ophthalmology — MCQs

On this page
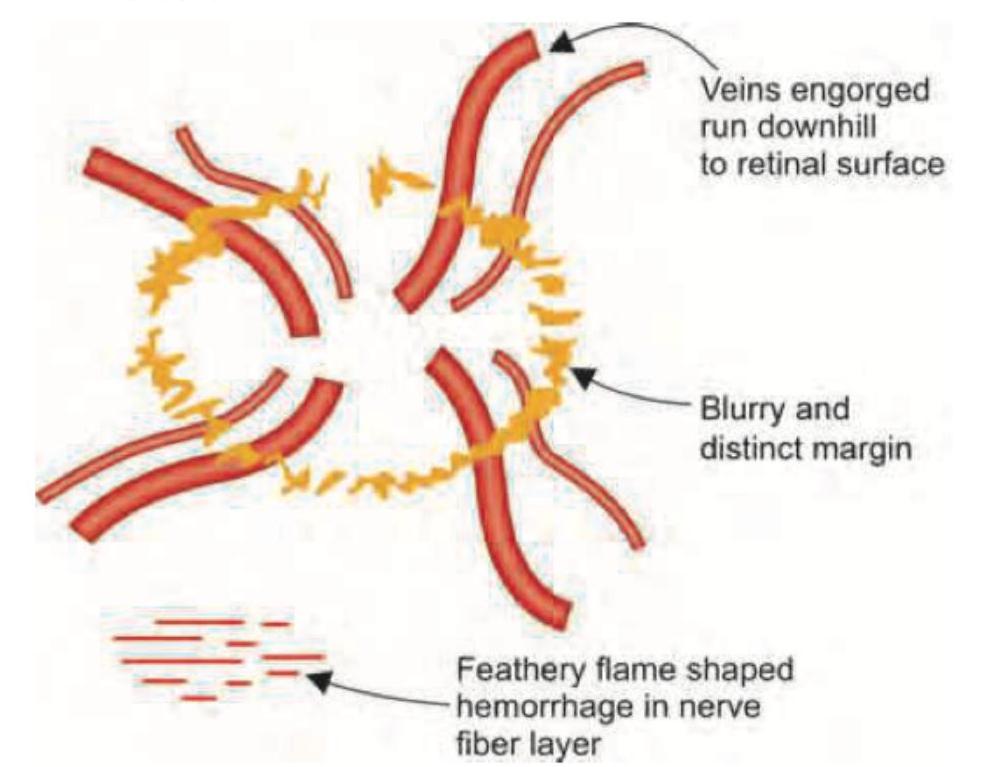
The given image shows which of the following conditions? (AIIMS Nov 2018)

The images show a normal optic disc (left) and papilledema with blurred disc margins (right). Which of the following can cause papilledema?
The following fundus finding is seen in:

Identify the visual field defect depicted by the boxed pair of diagrams at the bottom of the image. The left diagram represents the right eye (OD), the right diagram represents the left eye (OS), and the dark regions indicate visual field loss.

A 27-year-old female patient presents with sudden diminishing vision associated with a relative afferent pupillary defect in the right eye. On examination, the left eye is normal. Which of the following combinations of investigations would be most appropriate?
A 12-year-old boy is admitted to the emergency department with signs of meningitis. To determine the specific type of meningitis, it is necessary to aspirate cerebrospinal fluid with a lumbar puncture for laboratory examination. However, before performing a lumbar puncture, it must be established that the cerebrospinal fluid pressure is not elevated. What condition in the eye would indicate that cerebrospinal fluid pressure is too elevated for a lumbar puncture to be performed?
Most common optic nerve tumor in children causing blindness:
A case of injury to right brow due to a fall from scooter presents with sudden loss of vision in the right eye. The pupil shows absent direct reflex but a normal consensual pupillary reflex is present. The fundus is normal. The treatment of choice is:
Which of the following is NOT a feature of Horner's syndrome?
Enlargement of the blind spot occurs in which of the following
Practice by Chapter
Anatomy of Visual Pathways
Practice Questions
Pupillary Disorders
Practice Questions
Optic Neuritis
Practice Questions
Ischemic Optic Neuropathies
Practice Questions
Other Optic Neuropathies
Practice Questions
Papilledema
Practice Questions
Cranial Nerve Palsies
Practice Questions
Nystagmus
Practice Questions
Visual Field Defects
Practice Questions
Neuro-ophthalmic Manifestations of Intracranial Lesions
Practice Questions
Functional Visual Disorders
Practice Questions
Migraine and the Eye
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app