
Neuro-Ophthalmology — MCQs

On this page
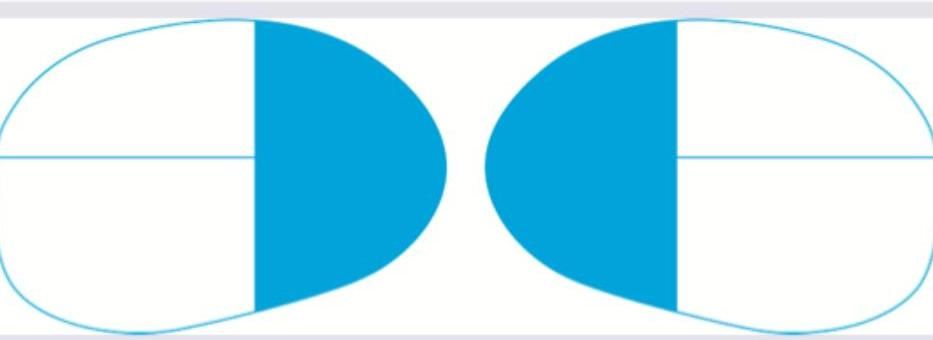
All are causes of the field defect shown below except:
All are causes for the visual defect shown below except:
The given fundus examination reveals presence of:
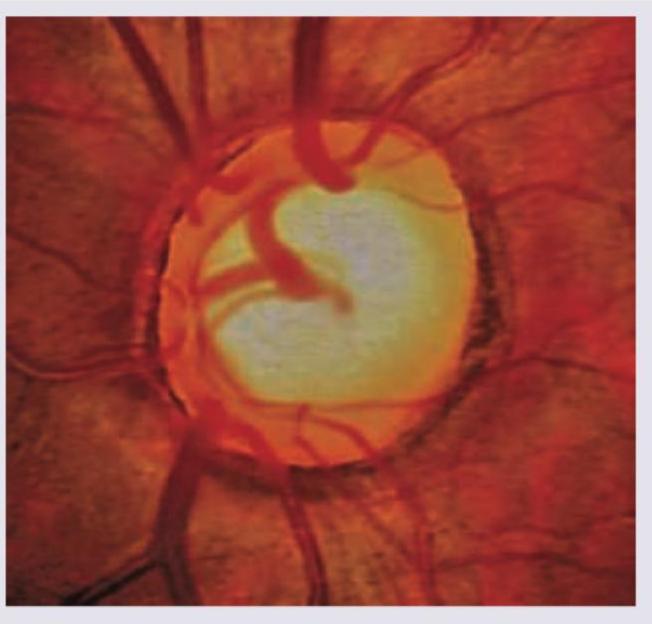
An 8-year-old child presents with gradual reduction in vision in the right eye. Family history of similar presentation was elicited on the maternal side. On examination, on right side direct light reflex is absent and consensual light reflex is present. Fundus examination was performed. What is the diagnosis?

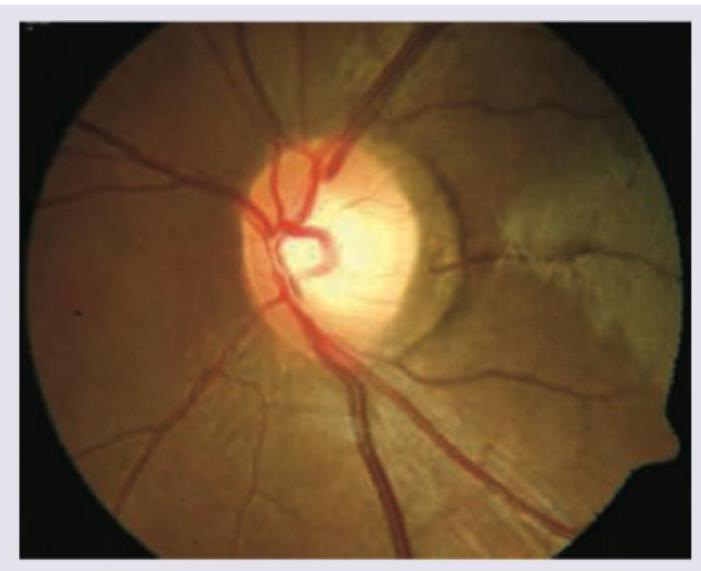
The following fundus finding is seen in:
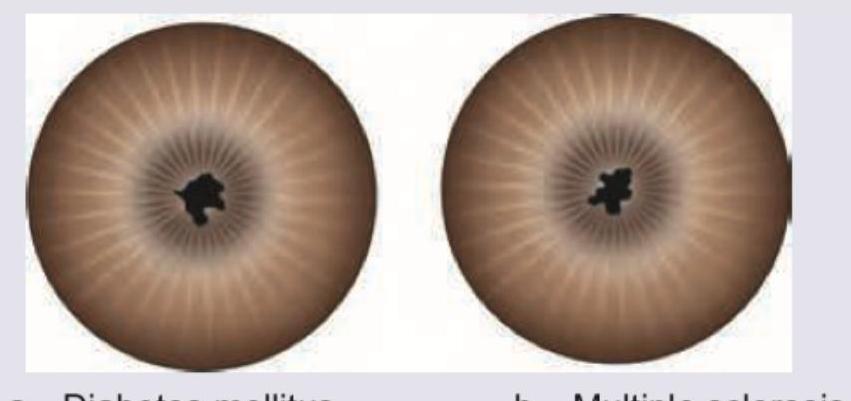
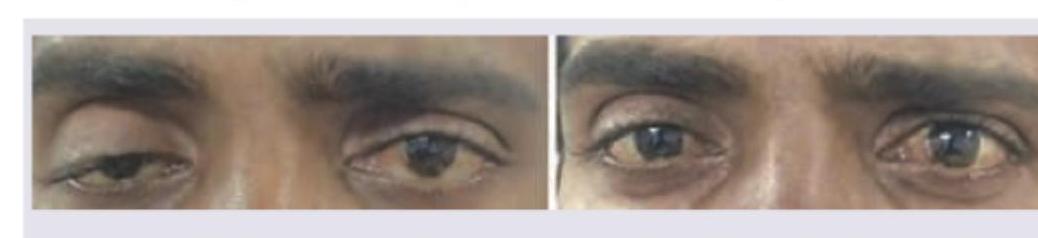
The pupils shown below demonstrate Argyll Robertson-like light-near dissociation: they are miotic, nonreactive to light, but reactive to accommodation. All of the following are recognized causes of this pupillary finding EXCEPT:
The following visual loss is seen due to lesion in:
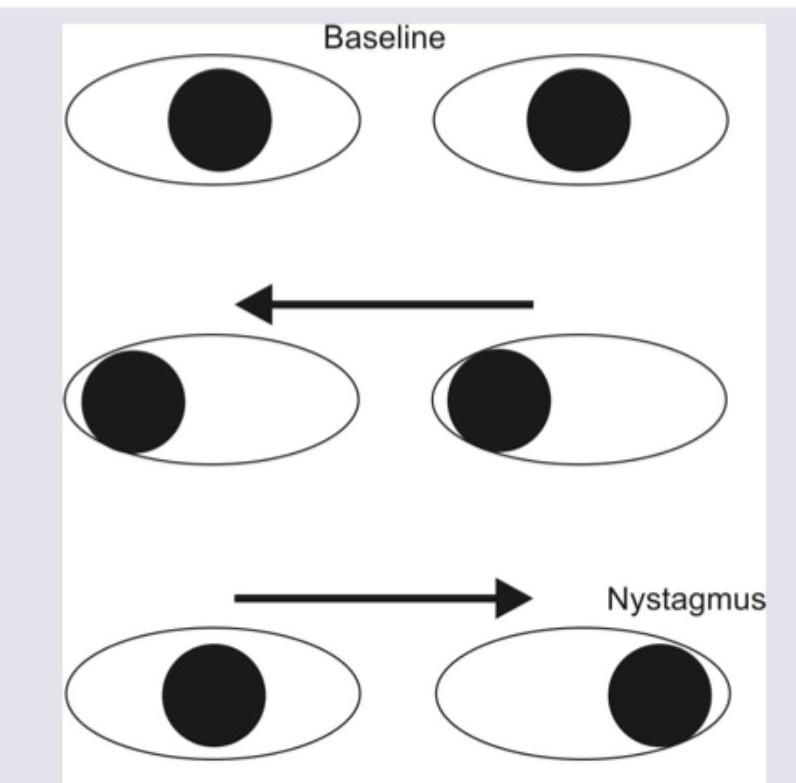
A patient presents with the eye movement abnormalities shown in the image below. What is the diagnosis?
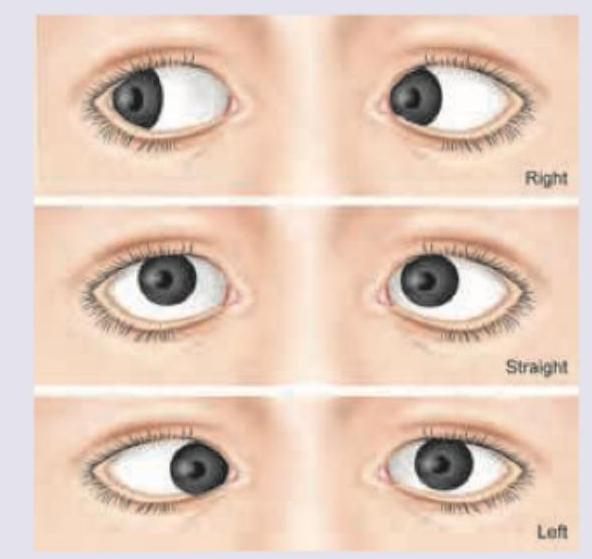
A 60-year-old male presents with horizontal diplopia that worsens on left gaze. The finding is shown in the image. Diagnosis is?
What is the diagnosis?
Practice by Chapter
Anatomy of Visual Pathways
Practice Questions
Pupillary Disorders
Practice Questions
Optic Neuritis
Practice Questions
Ischemic Optic Neuropathies
Practice Questions
Other Optic Neuropathies
Practice Questions
Papilledema
Practice Questions
Cranial Nerve Palsies
Practice Questions
Nystagmus
Practice Questions
Visual Field Defects
Practice Questions
Neuro-ophthalmic Manifestations of Intracranial Lesions
Practice Questions
Functional Visual Disorders
Practice Questions
Migraine and the Eye
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app