
Neuro-Ophthalmology — MCQs

On this page
What is the probable diagnosis for a patient who exhibits miosis, anhidrosis, mild ptosis, and a persistent small pupil even in low light conditions?
A patient presents with right-sided field defects in both eyes, but central vision remains unaffected. What is the most likely diagnosis?
Which of the following is NOT a feature of Horner's Syndrome?
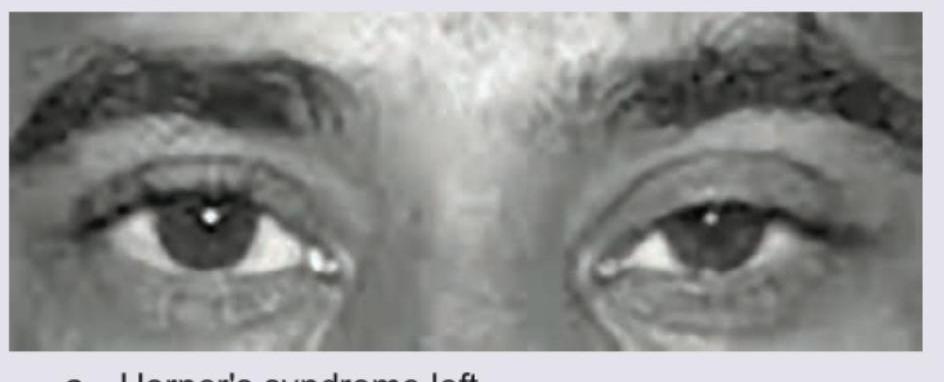
Which of the following is the diagnosis based on the given eye movement abnormality image?
In optic neuritis, which is true?
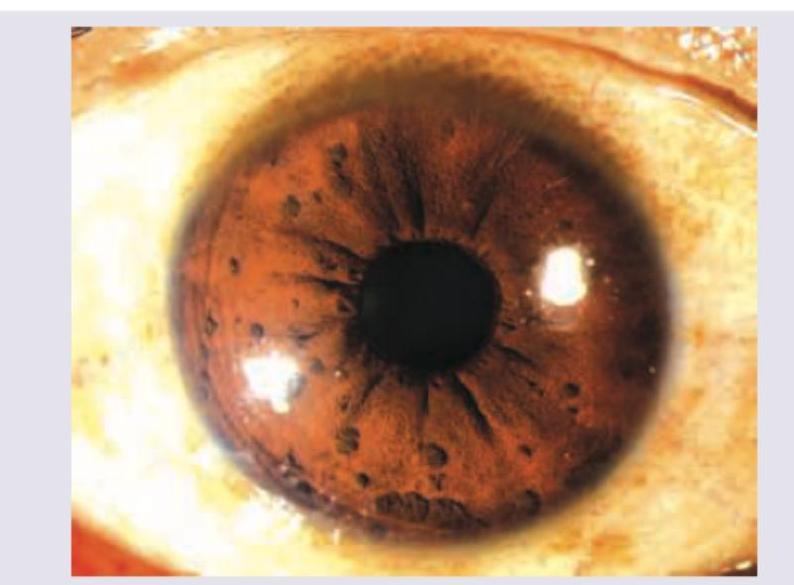
A 20-year-old woman is admitted with the following presentation. 1% pilocarpine is not showing any response on the side of mydriasis. What is the diagnosis? (Recent NEET Pattern 2016-17)
A child has been diagnosed with cavernous sinus meningioma. Which of these is correct?

The following image shows:
Which is the most likely diagnosis of this patient?
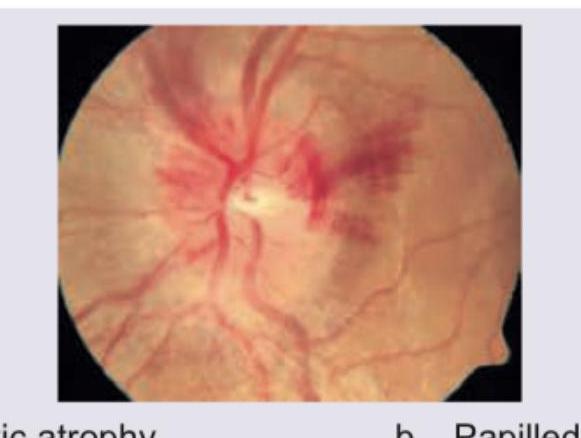
What is the diagnosis based on this fundus examination?
Practice by Chapter
Anatomy of Visual Pathways
Practice Questions
Pupillary Disorders
Practice Questions
Optic Neuritis
Practice Questions
Ischemic Optic Neuropathies
Practice Questions
Other Optic Neuropathies
Practice Questions
Papilledema
Practice Questions
Cranial Nerve Palsies
Practice Questions
Nystagmus
Practice Questions
Visual Field Defects
Practice Questions
Neuro-ophthalmic Manifestations of Intracranial Lesions
Practice Questions
Functional Visual Disorders
Practice Questions
Migraine and the Eye
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app