
Anatomy of Visual Pathways — MCQs

Ramkali bai, a 35-year-old female presented with a one-year history of menstrual irregularity and galactorrhoea. She also had off and on headache, her examination revealed bitemporal superior quadrantanopia. Her fundus examination showed primary optic atrophy. Which of the following is a most likely diagnosis in this case -
Keyhole-shaped visual field defect is seen in a lesion involving which of the following regions?
Which structure contains the second-order neurons in the optic pathway?
Identify the visual field defect shown in the image.

Visual processing center is located in -
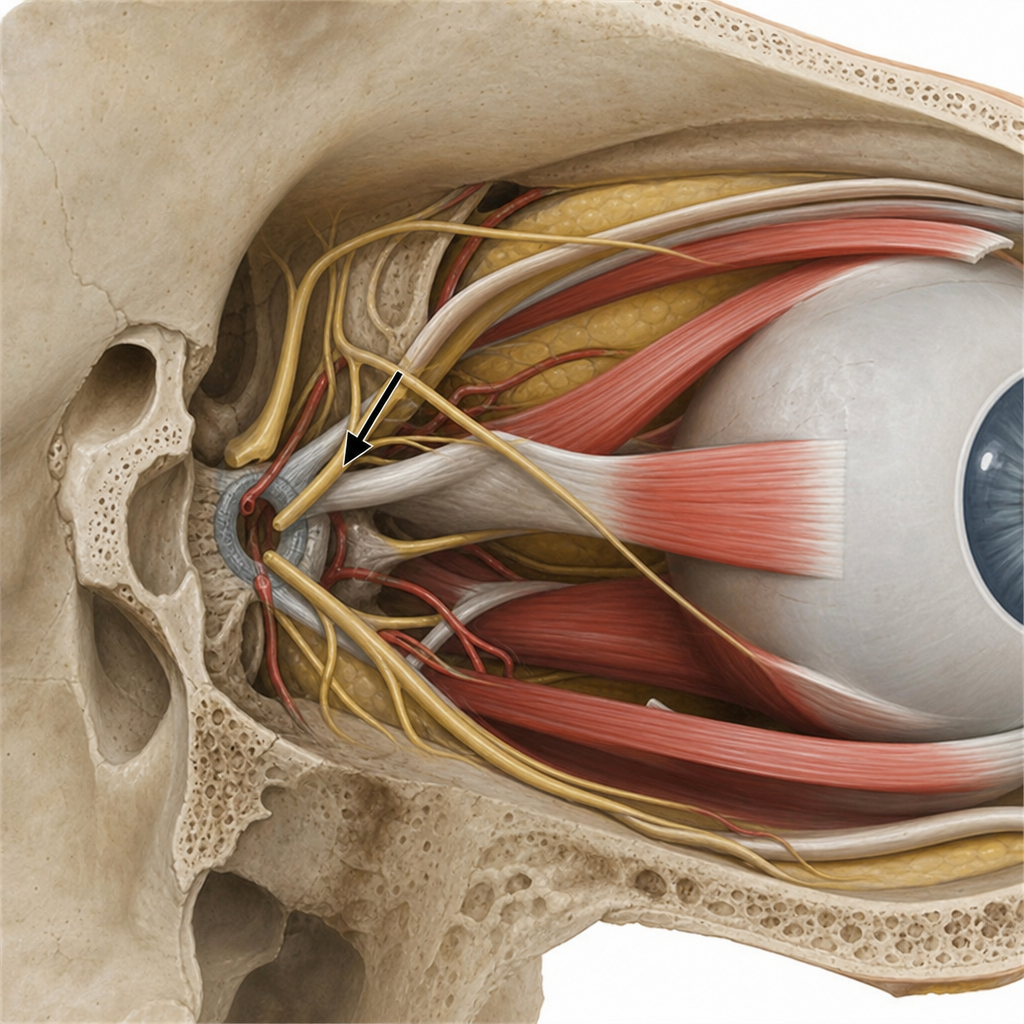
Lesion of the marked structure affects all EXCEPT
The fibers from the contralateral nasal hemiretina project to the following layers of the lateral geniculate nucleus:
Macular sparing is associated with lesions in:
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
Wernicke's hemianopic pupillary response is seen in lesion of-
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app