
Glaucoma — MCQs

On this page
In acute congestive glaucoma, what is the typical pupil appearance?
An elderly male with a history of glaucoma presents with a bulging cornea on examination. What is the most likely diagnosis?
Which of the following is NOT a triad of congenital glaucoma?
Glaucoma associated with intraocular tumors is due to which of the following mechanisms?
All of the following can precipitate an attack of narrow-angle glaucoma except:
What is the value of diurnal variation of intraocular pressure (IOP) above which a diagnosis of glaucoma can be made?
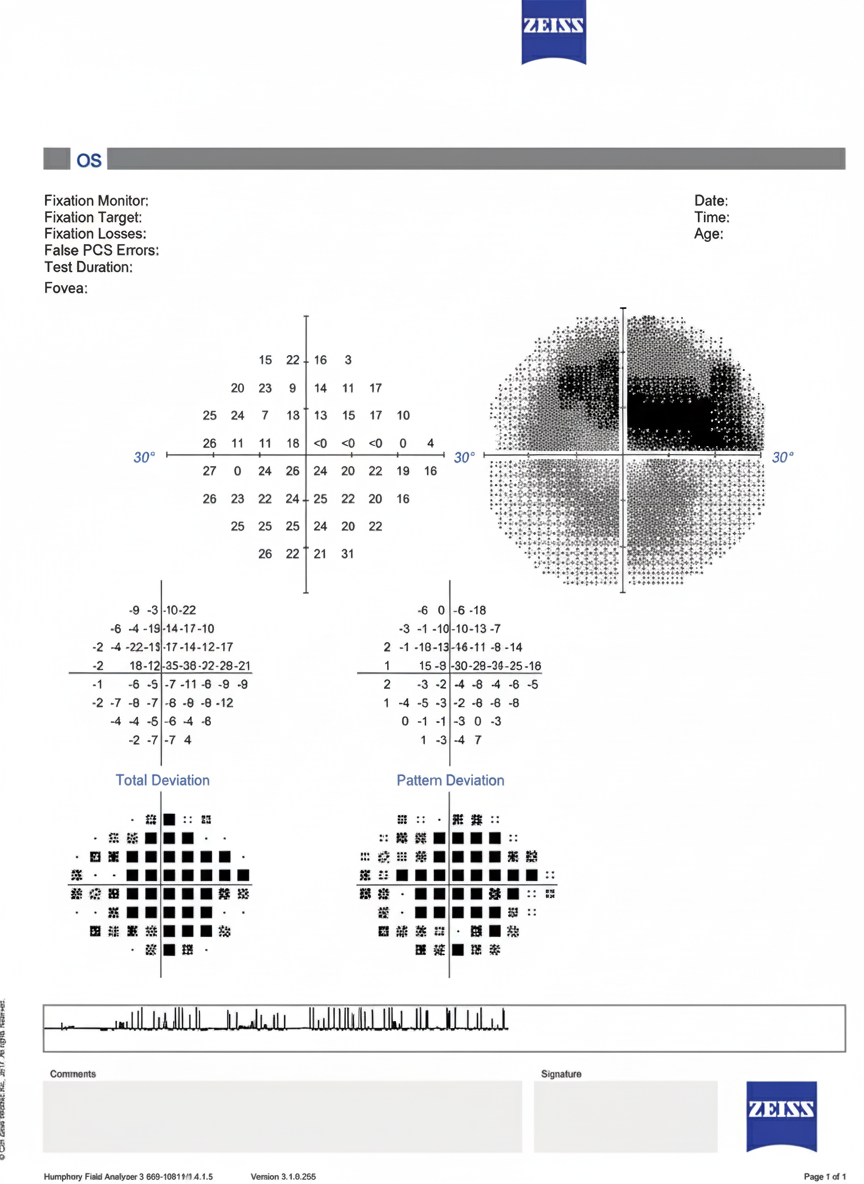
Which statement correctly describes the testing principle of automated static perimetry using the Humphrey Field Analyzer?
Schwalbe's line is:
A young male presents with painless loss of vision and an intraocular pressure of 60mm Hg. Which of the following is the most likely diagnosis?
Which of the following tonometers can be used in a diseased cornea?
Practice by Chapter
Aqueous Humor Dynamics
Practice Questions
Primary Open-Angle Glaucoma
Practice Questions
Primary Angle-Closure Glaucoma
Practice Questions
Secondary Open-Angle Glaucomas
Practice Questions
Secondary Angle-Closure Glaucomas
Practice Questions
Developmental and Congenital Glaucomas
Practice Questions
Medical Management of Glaucoma
Practice Questions
Laser Therapy in Glaucoma
Practice Questions
Glaucoma Filtration Surgery
Practice Questions
Glaucoma Drainage Devices
Practice Questions
Angle Assessment Techniques
Practice Questions
Visual Field Testing in Glaucoma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app