
Glaucoma — MCQs

On this page
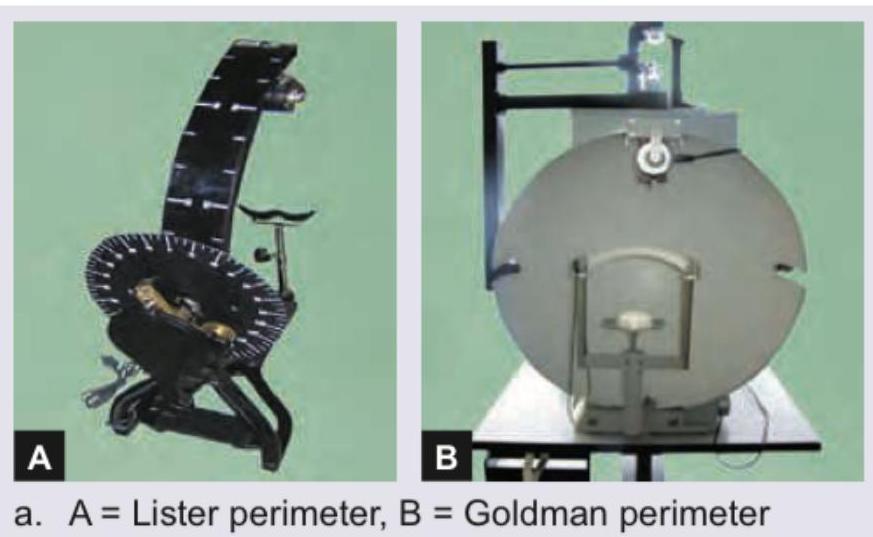
Identify the instrument shown:
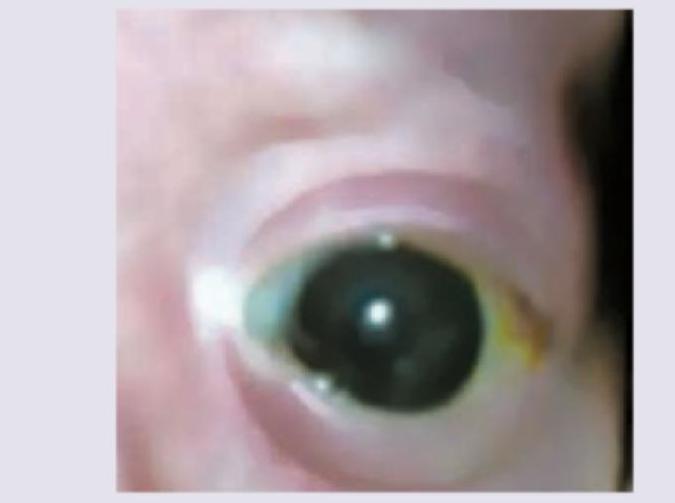
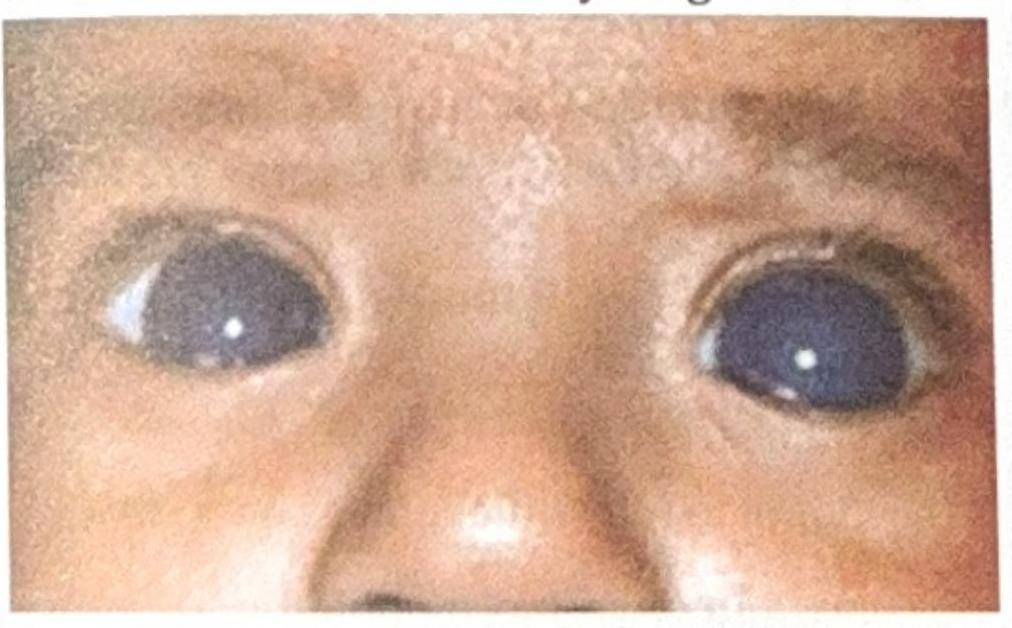
A 2-year-old child is brought with complaints of watering of eyes, photophobia and intermittently keeping eyes closed while watching TV. What may be the diagnosis? (AIIMS Nov 2018)

Select the FALSE statement pertaining to the disease depicted in this picture. (AP PG 2016)
The normal range of intraocular pressure (in mmHg) is
A patient presents with eye ache and difficulty in vision after watching a movie. What will be the first line of management?
A one-month-old baby presents with excessive tearing (watering) and an increased corneal size. What is the most likely diagnosis?
Which triad is seen after an acute attack of angle-closure glaucoma?
What is the earliest change in glaucoma on perimetry?
Which of the following lens is used in direct gonioscopy?
A 30-year-old female presents with redness and pain in the eye. Examination revealed 38 mm of Hg on IOP, aqueous flare, and corneal precipitates. Which of the following drugs must be avoided for her?
Practice by Chapter
Aqueous Humor Dynamics
Practice Questions
Primary Open-Angle Glaucoma
Practice Questions
Primary Angle-Closure Glaucoma
Practice Questions
Secondary Open-Angle Glaucomas
Practice Questions
Secondary Angle-Closure Glaucomas
Practice Questions
Developmental and Congenital Glaucomas
Practice Questions
Medical Management of Glaucoma
Practice Questions
Laser Therapy in Glaucoma
Practice Questions
Glaucoma Filtration Surgery
Practice Questions
Glaucoma Drainage Devices
Practice Questions
Angle Assessment Techniques
Practice Questions
Visual Field Testing in Glaucoma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app