
Glaucoma — MCQs

On this page
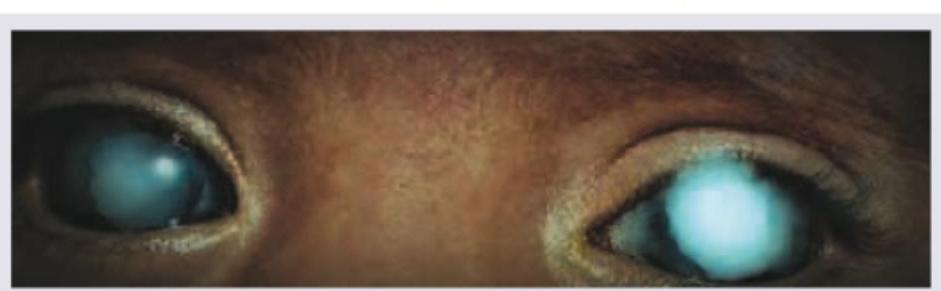
Which of the following is incorrect about a 2-yearold child presenting with watering from both eyes?
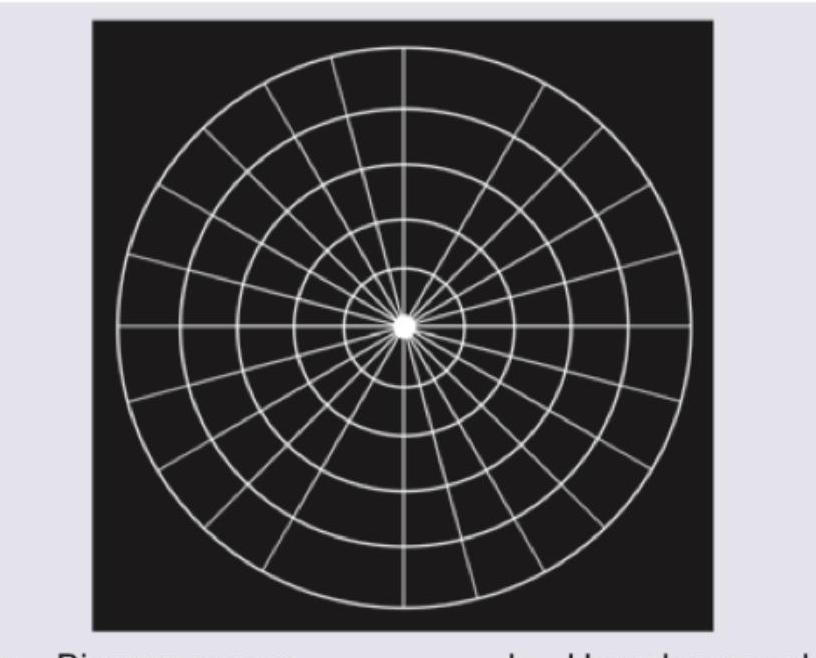
Which of the following methods of visual field testing is shown below?
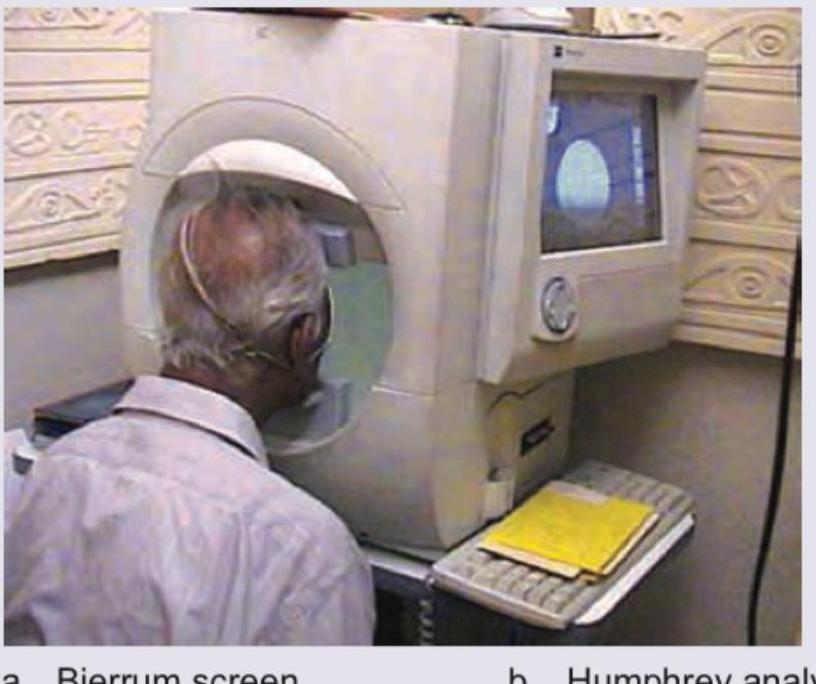
Which method of visual field testing is shown below?
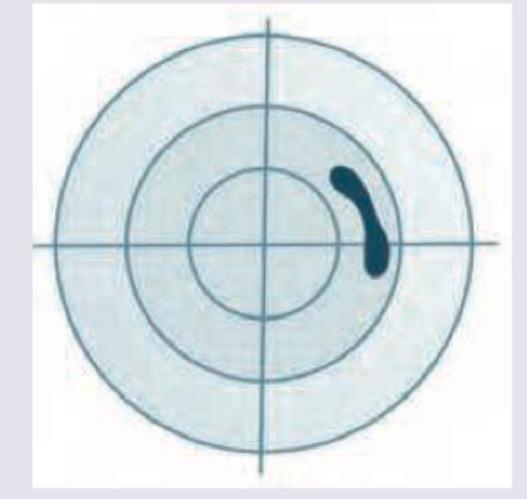
Which field defect is shown in the image below?

Which of the given field defects is shown in the image given below?
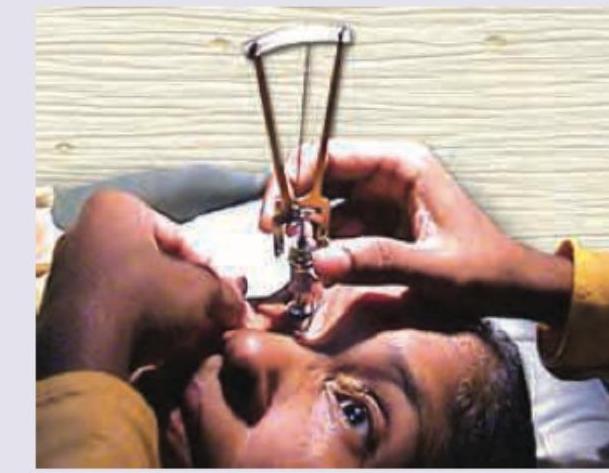
What is the test being performed in the image shown below?

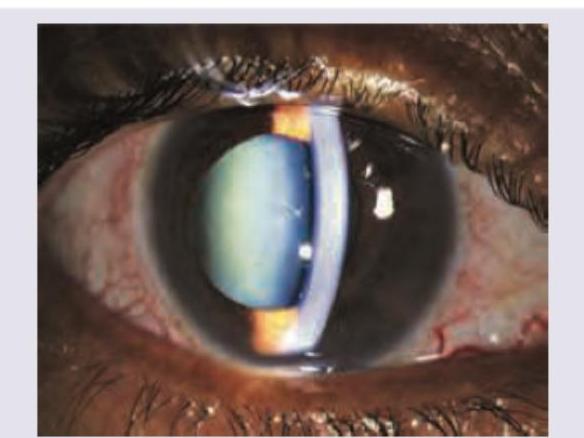
A 25 -year-old lady with past history of seeing colored haloes was watching a movie in a theater when she started having right eye pain. She started feeling nauseous and had to leave the movie midway due to vomiting. On examination she is found to have ciliary and conjunctival congestion and the pupil is vertically oval. The picture of the eye is given below. All are true about the condition shown except:
Name the test being performed in the image shown below:
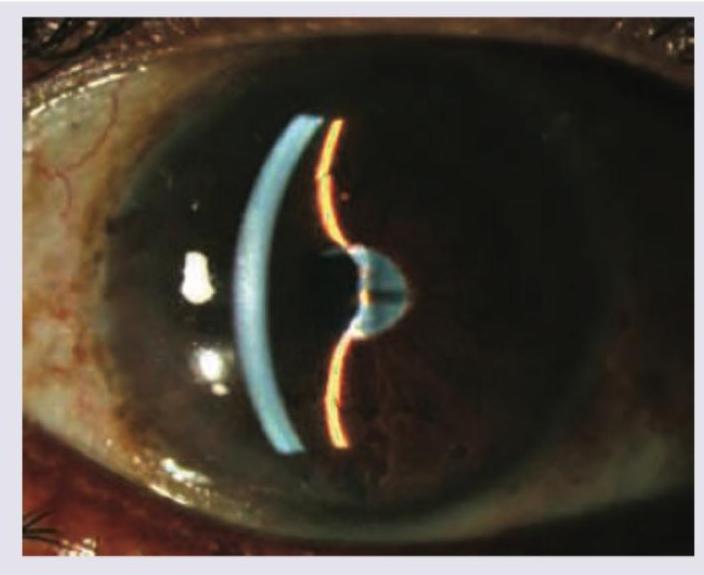
Which of the following is responsible for abnormal shape of anterior chamber shown below?
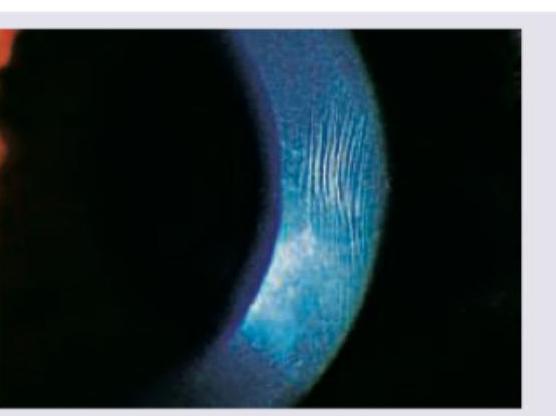
These vertical striations in the cornea shown below are seen in: (Recent NEET Pattern 2016-17)
Practice by Chapter
Aqueous Humor Dynamics
Practice Questions
Primary Open-Angle Glaucoma
Practice Questions
Primary Angle-Closure Glaucoma
Practice Questions
Secondary Open-Angle Glaucomas
Practice Questions
Secondary Angle-Closure Glaucomas
Practice Questions
Developmental and Congenital Glaucomas
Practice Questions
Medical Management of Glaucoma
Practice Questions
Laser Therapy in Glaucoma
Practice Questions
Glaucoma Filtration Surgery
Practice Questions
Glaucoma Drainage Devices
Practice Questions
Angle Assessment Techniques
Practice Questions
Visual Field Testing in Glaucoma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app