
Glaucoma — MCQs

On this page
Haab's striae are seen in which of the following conditions?
Malignant glaucoma is characterized by which of the following?
In angle closure glaucoma, what mainly causes obstruction to the outflow of aqueous humor?
All of the following causes coloured halos except?
An elderly female presents with sudden onset of pain, redness, and decreased vision. On examination, hazy cornea, fixed mid-dilated pupil, and shallow anterior chamber are noted. What is the diagnosis?
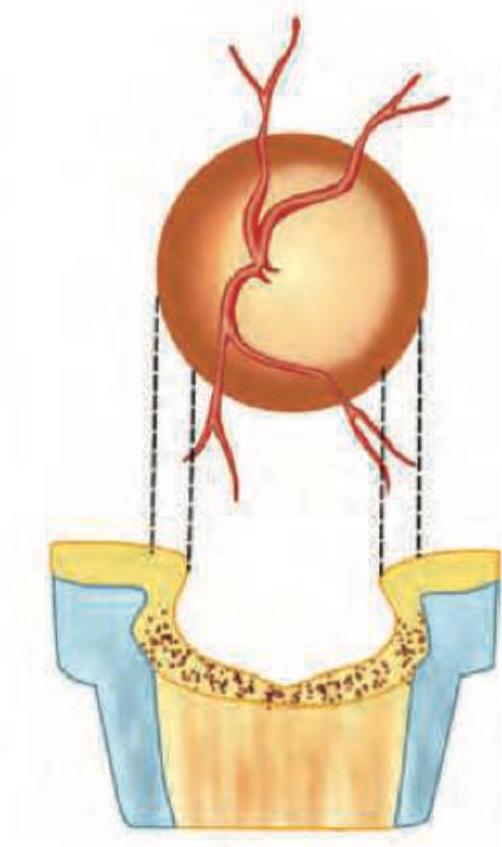
The image shows the following findings: Cupping of disc, Double angulation of blood vessels (visible in middle), one in steep wall of excavation and second in floor of the cup. Nasal shifting of vessels. Thinning of neural rim on temporal side.
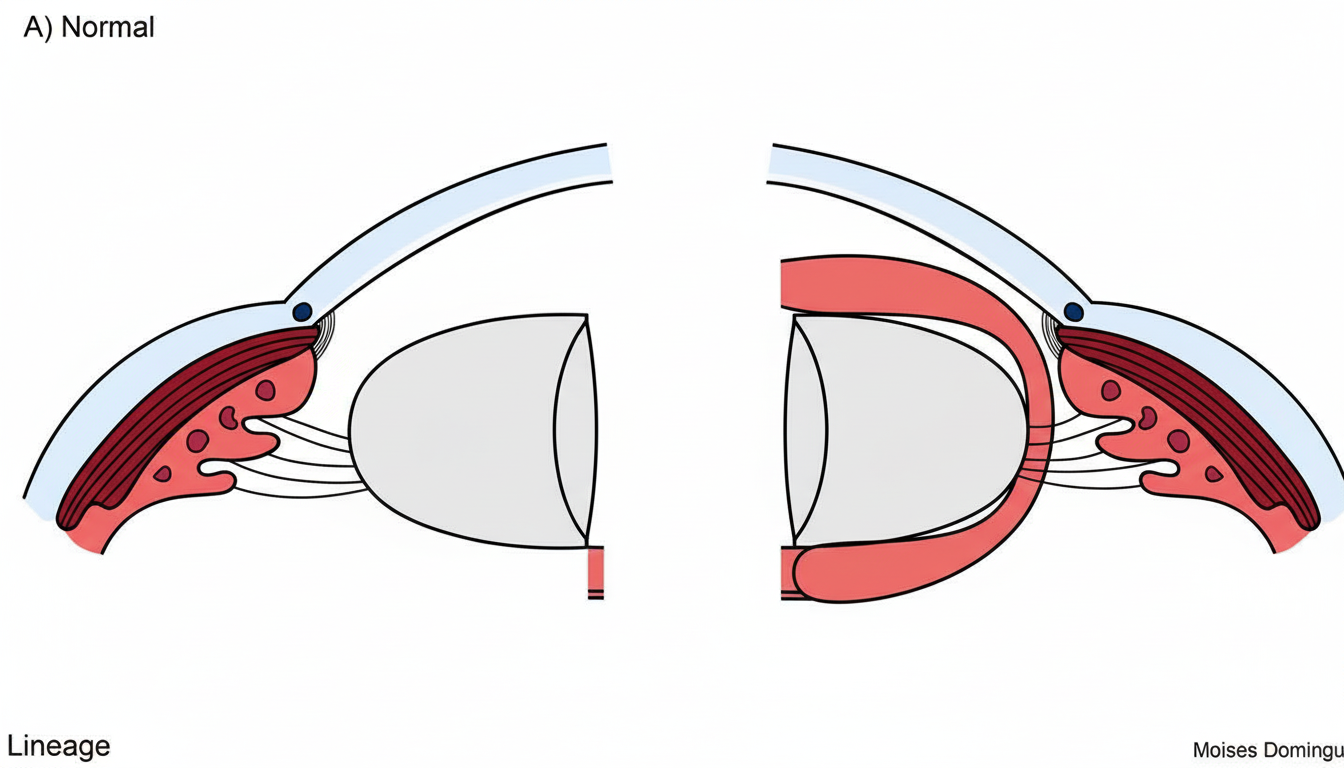
The image shows a funnel shaped anterior chamber (deeper in the center and narrow in the periphery), which is seen in angle closure glaucoma. This is caused by:
The image shows a tonometer being used. The principle of this device is Imbert-Fick's law, which measures IOP by flattening the cornea over a specific area with diameter of 3.06 mm. The values recorded are not influenced by scleral rigidity. What type of tonometry is being demonstrated in the image?

A patient with cataract presents with pain and redness of eye. On examination he had deep anterior chamber. What is the diagnosis?
Comment on the diagnosis:

Practice by Chapter
Aqueous Humor Dynamics
Practice Questions
Primary Open-Angle Glaucoma
Practice Questions
Primary Angle-Closure Glaucoma
Practice Questions
Secondary Open-Angle Glaucomas
Practice Questions
Secondary Angle-Closure Glaucomas
Practice Questions
Developmental and Congenital Glaucomas
Practice Questions
Medical Management of Glaucoma
Practice Questions
Laser Therapy in Glaucoma
Practice Questions
Glaucoma Filtration Surgery
Practice Questions
Glaucoma Drainage Devices
Practice Questions
Angle Assessment Techniques
Practice Questions
Visual Field Testing in Glaucoma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app