
Glaucoma — MCQs

On this page
Hypermature morgagnian cataract most commonly leads to which type of glaucoma?
Increased intraocular tension is seen in all except?
What is the earliest visual field change in open-angle glaucoma?
Tonography helps determine which of the following?
Neovascular glaucoma is not seen in which of the following conditions?
Triple surgery in glaucoma includes all of the following except?
Which of the following conditions is the drug of choice for a topical beta blocker?
Pilocarpine reduces intraocular pressure in persons with closed-angle glaucoma by:
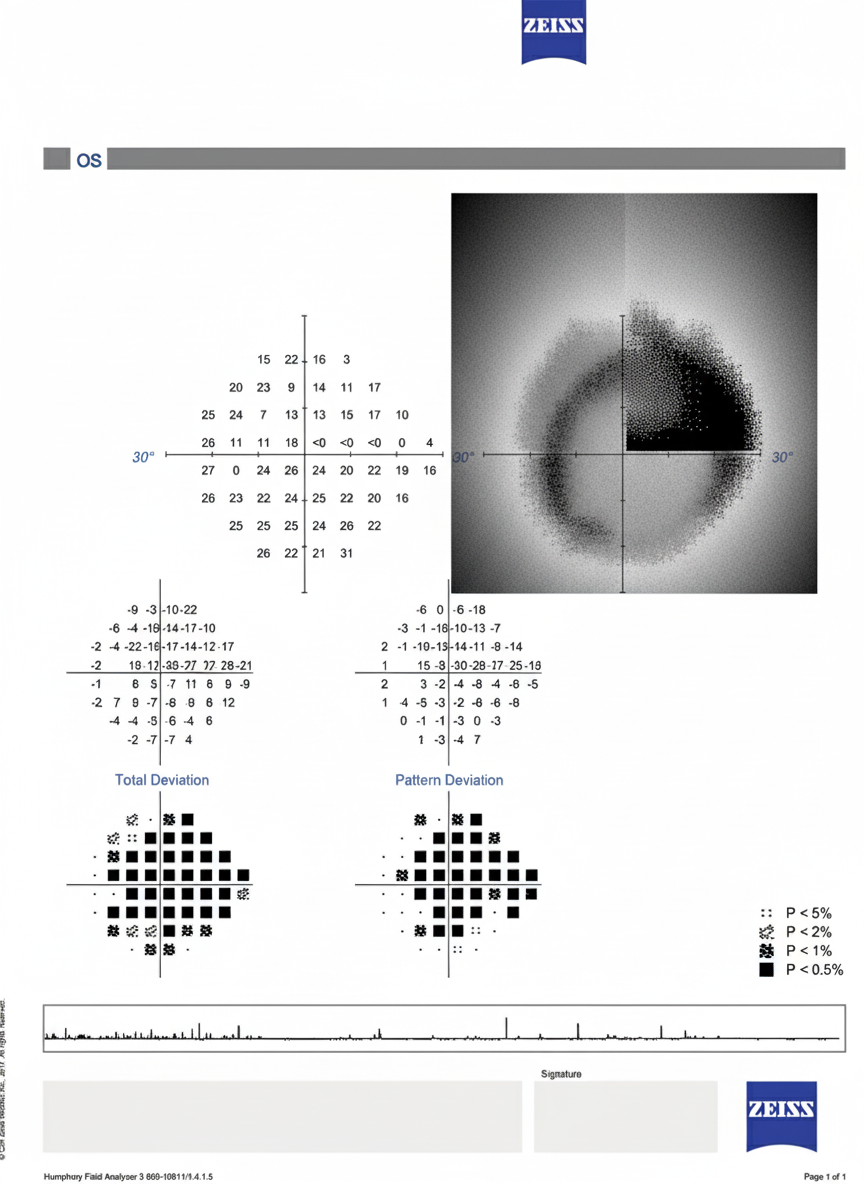
Based on the perimetry result print-out, what is the most likely diagnosis?
What is the ideal treatment for subacute angle closure glaucoma?
Practice by Chapter
Aqueous Humor Dynamics
Practice Questions
Primary Open-Angle Glaucoma
Practice Questions
Primary Angle-Closure Glaucoma
Practice Questions
Secondary Open-Angle Glaucomas
Practice Questions
Secondary Angle-Closure Glaucomas
Practice Questions
Developmental and Congenital Glaucomas
Practice Questions
Medical Management of Glaucoma
Practice Questions
Laser Therapy in Glaucoma
Practice Questions
Glaucoma Filtration Surgery
Practice Questions
Glaucoma Drainage Devices
Practice Questions
Angle Assessment Techniques
Practice Questions
Visual Field Testing in Glaucoma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app