
Scleritis: Anterior — MCQs

Recurrent anterior uveitis with increased intraocular tension is seen in which of the following conditions?
In a patient with acute anterior uveitis presenting with raised intraocular pressure, the PRIMARY treatment should be:
A 40-year-old woman with rheumatoid arthritis presents with eye pain and redness. Examination reveals scleritis. What is the most likely associated systemic complication?
Most common type of scleritis is
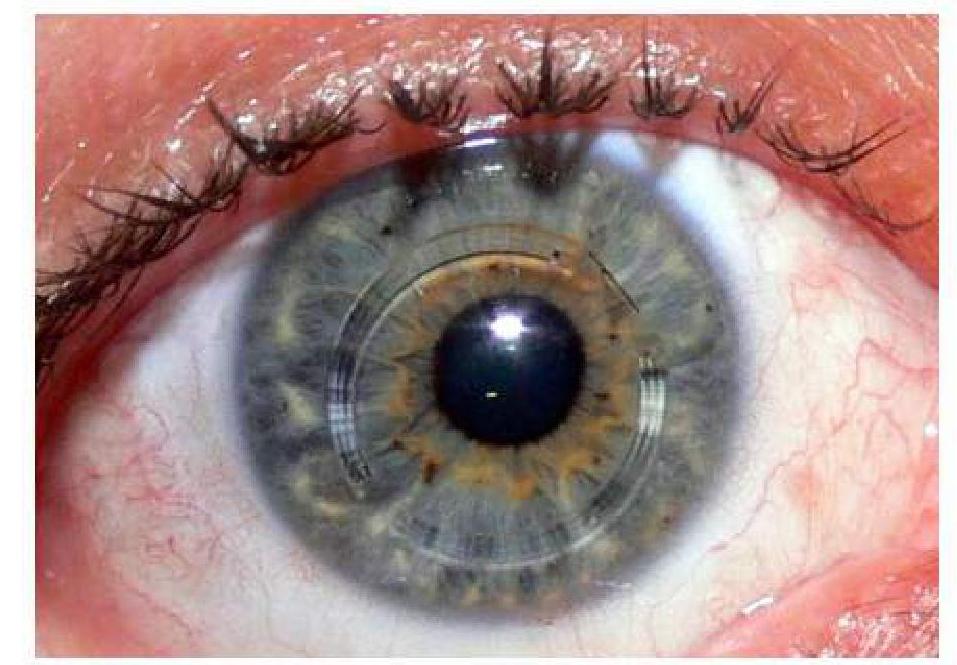
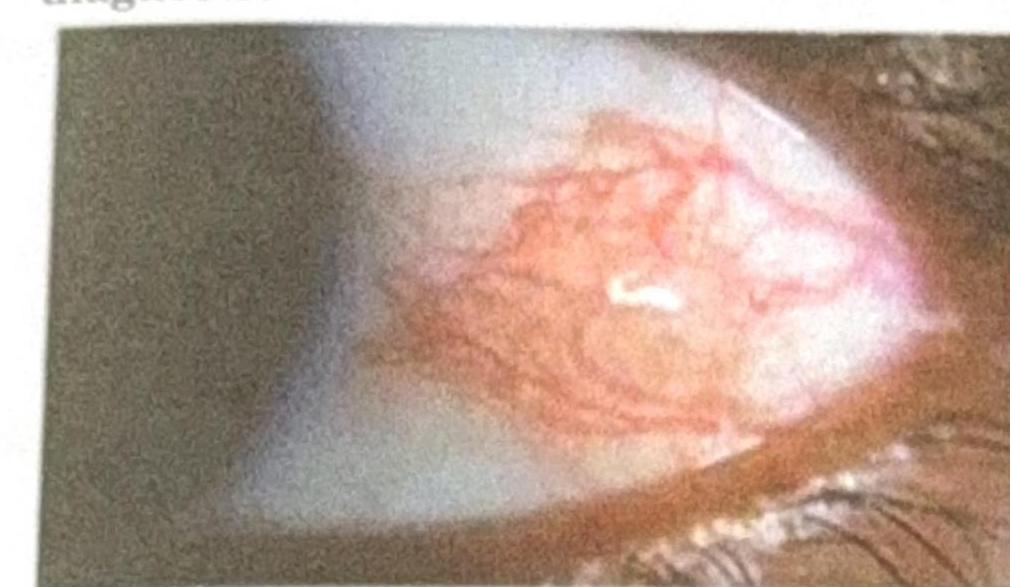
A patient presents with a nodular swelling near the limbus, which does not blanch with topical vasoconstrictors and recurs after treatment. Based on the image and clinical presentation, what is the most probable diagnosis?
Ciliary staphyloma occurs due to all of the following except:
Massaging of nasolacrimal duct is done in ?
Ciliary staphyloma is seen in which of the following conditions?
Which of the following is the MOST common type of staphyloma in myopia?
What is an intercalary staphyloma?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app