
Diseases of the Sclera — MCQs

On this page
Scleritis is commonly seen with which of the following conditions?
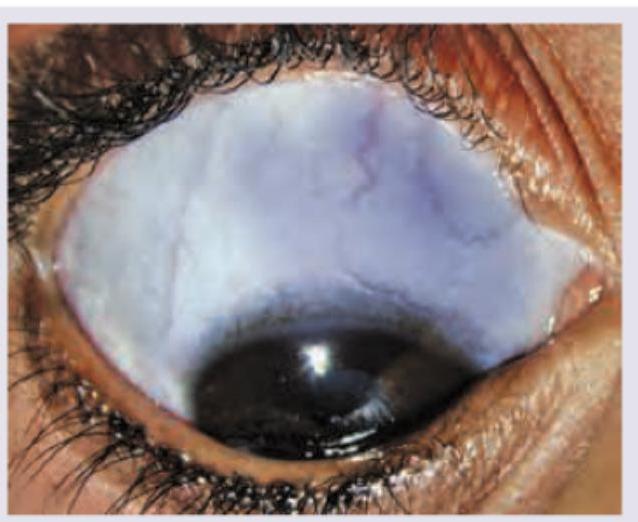
Blue coloured sclera is frequently associated with which of the following conditions?
Ciliary staphyloma affects the ciliary zone up to how many mm behind the limbus?
Which of the following is NOT true about scleritis?
Blue sclera is seen in which of the following conditions?
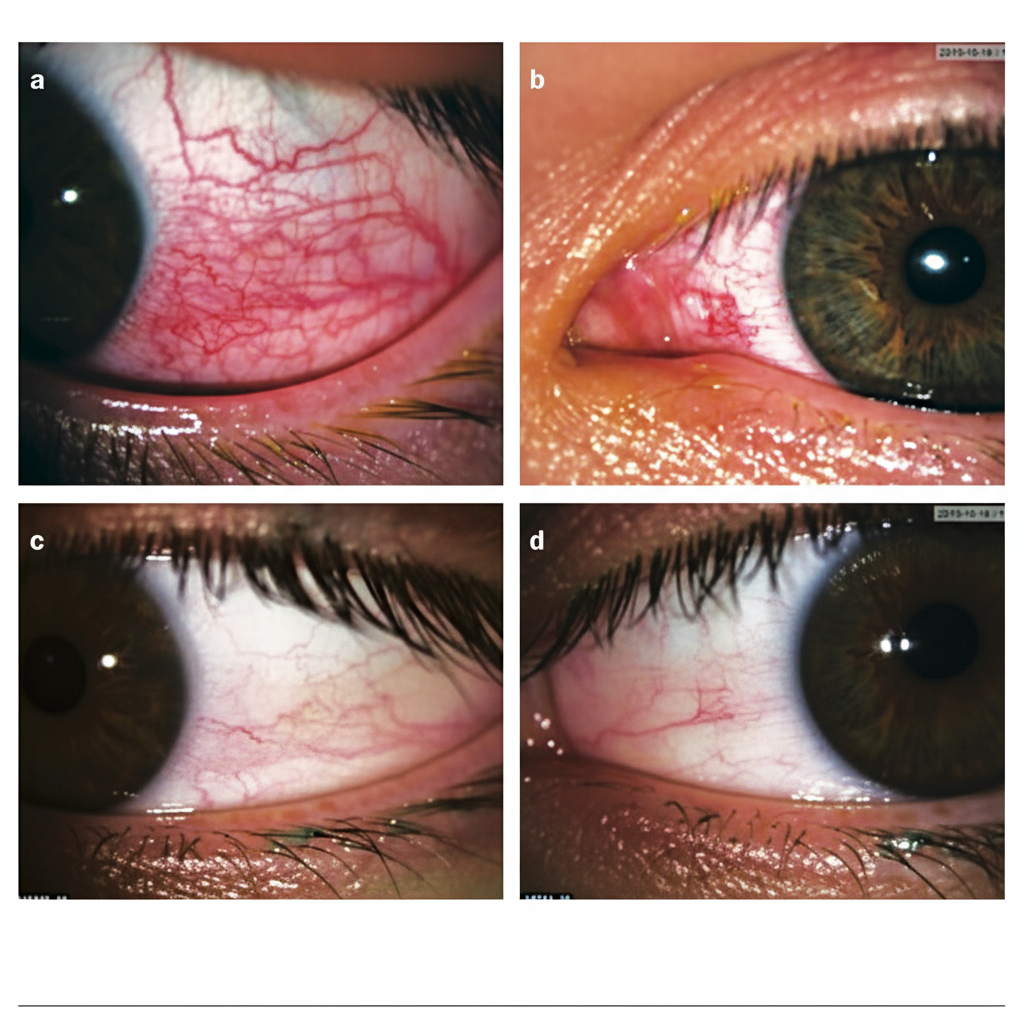
All are causes of the presentation shown below except:
A 25 -year-old patient presents with localized redness in right eye as shown below. On instillation of 10% phenylephrine there is quick blanching of the vessels. What is the diagnosis?
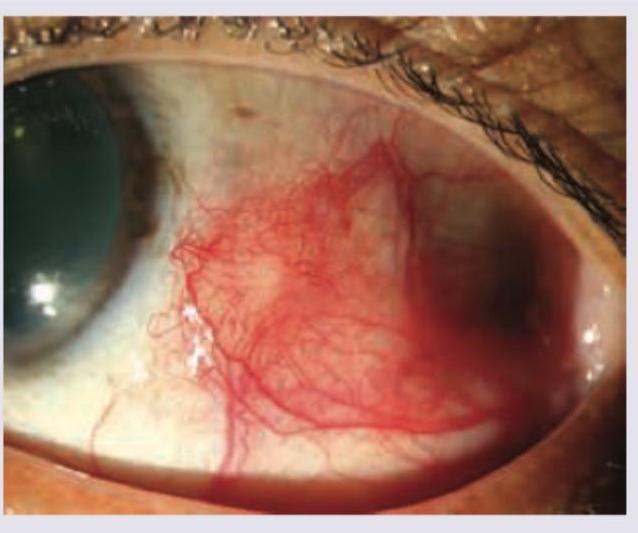
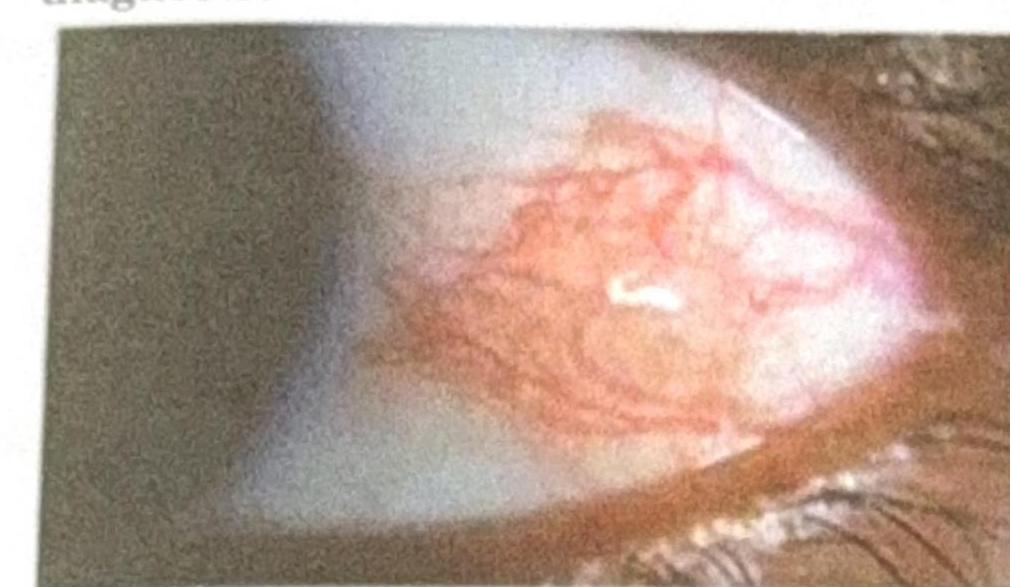
A patient presents with a nodular swelling near the limbus, which does not blanch with topical vasoconstrictors and recurs after treatment. Based on the image and clinical presentation, what is the most probable diagnosis?
The given image shows blanching of vascularity after the phenylephrine use. What is the likely diagnosis?
Posterior staphyloma is seen in -
Practice by Chapter
Anatomy and Physiology of Sclera
Practice Questions
Episcleritis
Practice Questions
Scleritis: Anterior
Practice Questions
Scleritis: Posterior
Practice Questions
Infectious Scleritis
Practice Questions
Scleral Manifestations of Systemic Disease
Practice Questions
Blue Sclera Syndromes
Practice Questions
Scleral Degenerations
Practice Questions
Scleral Trauma
Practice Questions
Scleral Surgeries
Practice Questions
Necrotizing Scleritis
Practice Questions
Staphyloma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app