
Diseases of the Retina — MCQs

On this page
A 45-year-old diabetic presents with sudden painless vision loss. Cotton wool spots and dot hemorrhages seen. HbA1c is 9.2. Most likely diagnosis?
True about hydroxychloroquine retinopathy EXCEPT:
Following are the causes of sudden loss of vision except?
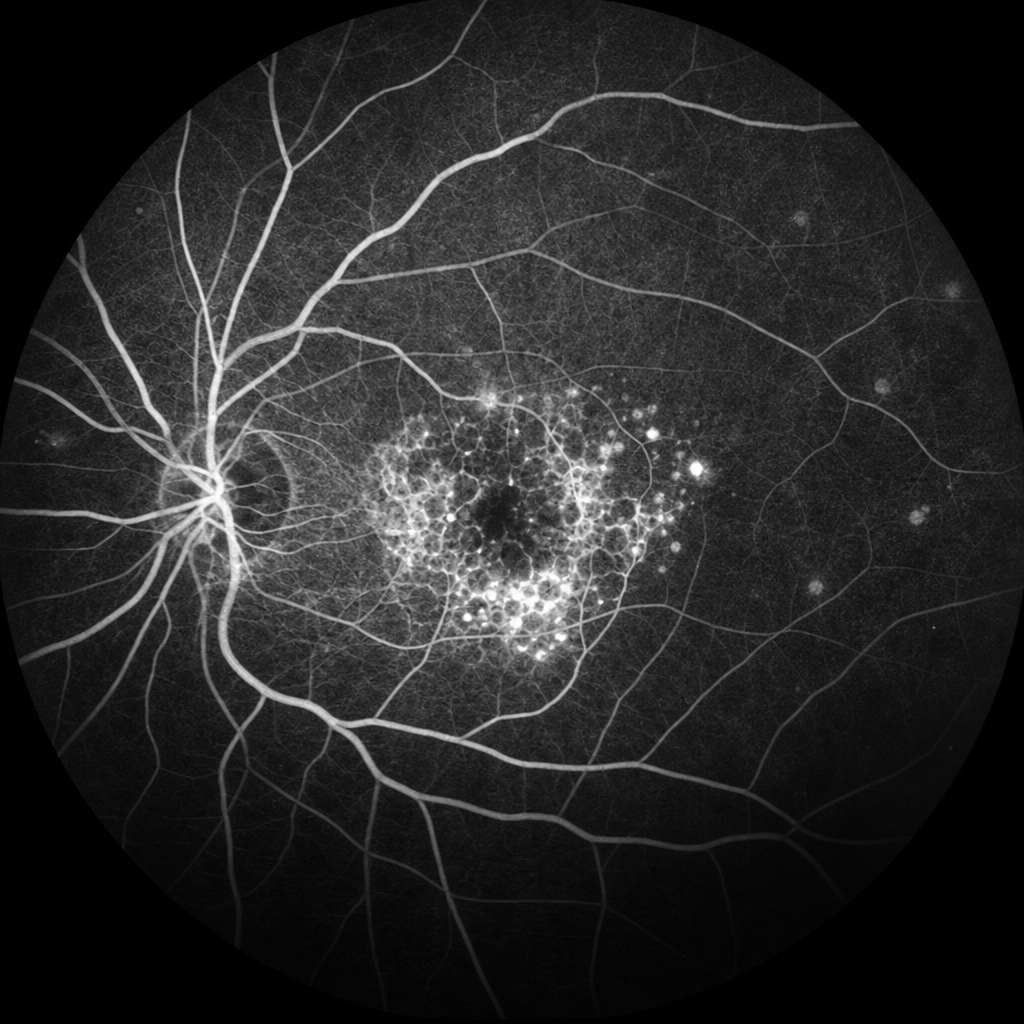
A patient with hypertension and diabetes presents with blurred vision. Fluorescein angiography shows the following findings. What is the diagnosis?
What is a characteristic fundoscopic finding in advanced hypertensive retinopathy?
A 30-year-old female presents with night blindness and peripheral vision loss. Likely diagnosis?
Assertion: Myopia is a risk factor for retinal detachment. Reason: In myopia, the axial length of the eye increases, causing the retina to thin and become more prone to detachment.
A patient presents with a central scotoma and metamorphopsia. What is the most likely cause?
A patient presents with superior quadrant vision loss since one week. Patient has Rheumatic Heart Disease (RHD) and is not taking medications. What is the most likely diagnosis?
A 40-year-old male experiences flashes of light. Which of the following can likely be the reason?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app