
Diseases of the Retina — MCQs

On this page
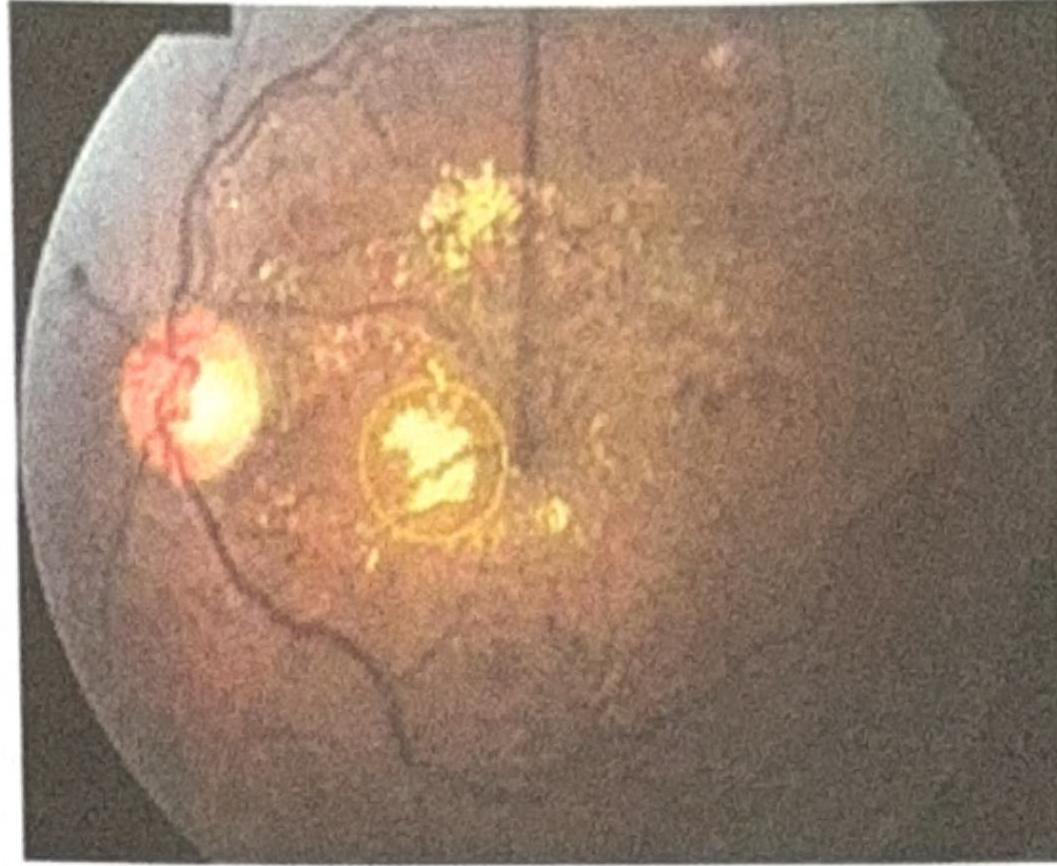
An elderly woman with a known history of diabetes presented with gradual painless diminution of vision. The fundus picture is shown below. What is the most likely diagnosis?
A child presenting with a whitish pupillary reflex (leukocoria) was treated with enucleation. Histopathology of the specimen showed Flexner-Wintersteiner rosettes. What is the most likely diagnosis?
What is the most common route of the spread of retinoblastoma?
A 58-year-old woman is brought to the emergency room by her husband complaining, “I can’t see out of my right eye.” She was watching television last night when she covered her left eye due to an itch and discovered that she could not see. The patient denies any precipitating event, pain, swelling, flashes, floaters, or headaches. Her past medical history is significant for uncontrolled hypertension and angina. Her medications include hydrochlorothiazide, lisinopril, atorvastatin, and nitroglycerin as needed. Her physical examination is unremarkable. Fundus examination demonstrates generalized pallor and slight disc edema with no hemorrhages. What is the most likely explanation for this patient’s symptoms?
A fundus examination shows 'sunset glow' appearance. Which fluorescein angiography finding would best support Vogt-Koyanagi-Harada disease?
A child presents with night blindness, delayed dark adaptation. Which investigation is to be done further to confirm the diagnosis?
Optic disc changes of retinitis pigmentosa:
Cause of sudden loss of vision in a diabetic is due to:
Which of the following is seen in retinitis pigmentosa?
Arden index is related to
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app