
Diseases of the Retina — MCQs

On this page
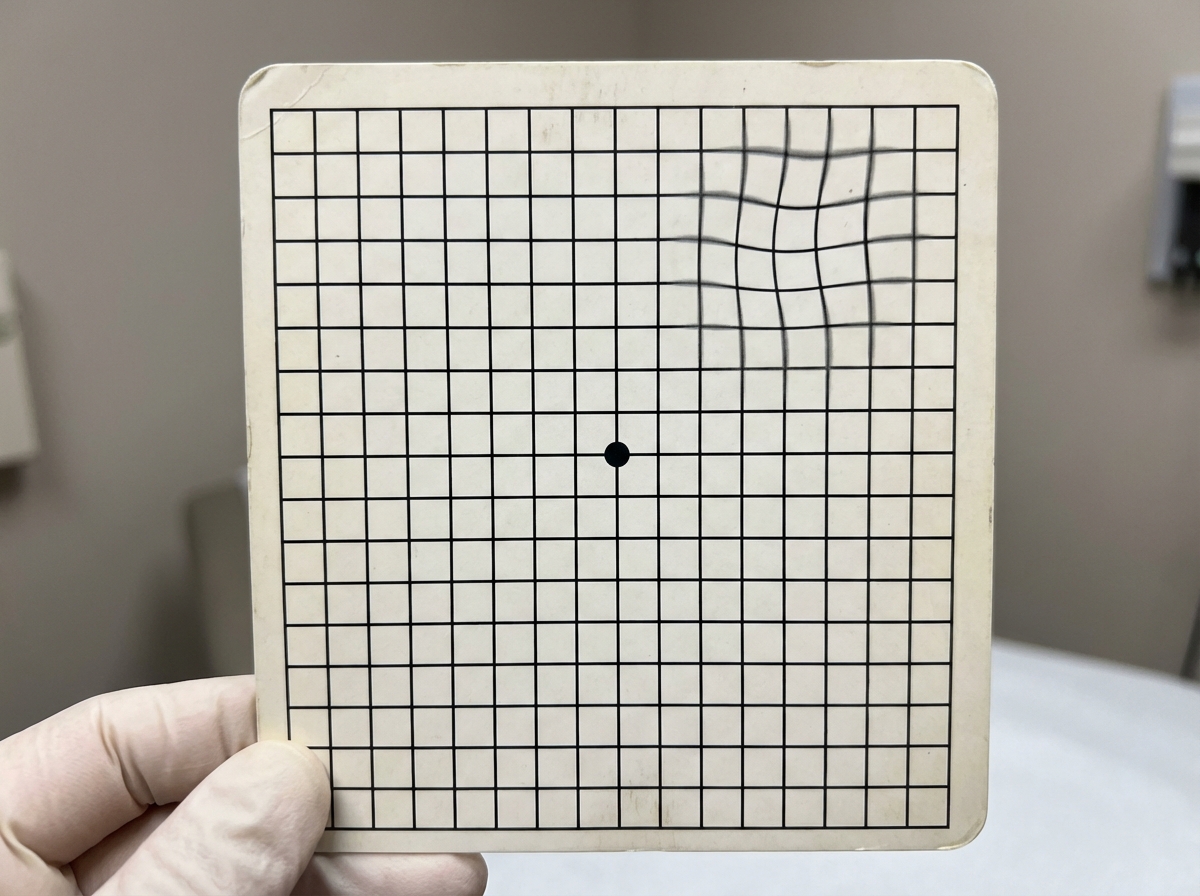
The test shown below is used for the evaluation of
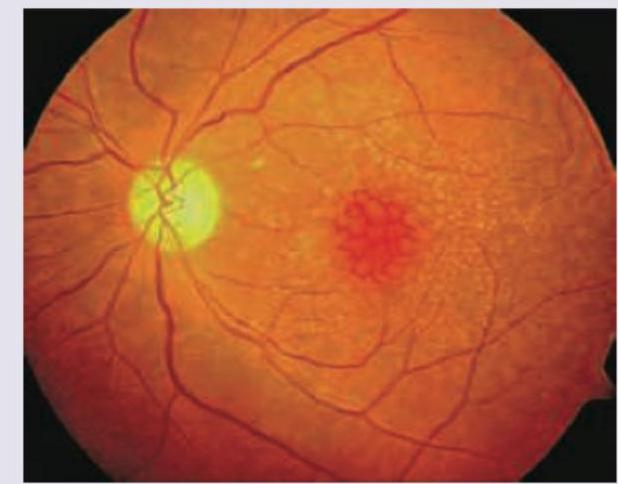
A 75-year-old Englishman living in India presents to OPD with complaints of gradual onset painless, progressive blurring of central vision. He says he could earlier drive to the hospital by himself but is not able to do so now. Slit lamp examination is normal. Fundus examination is given below. What is the diagnosis?
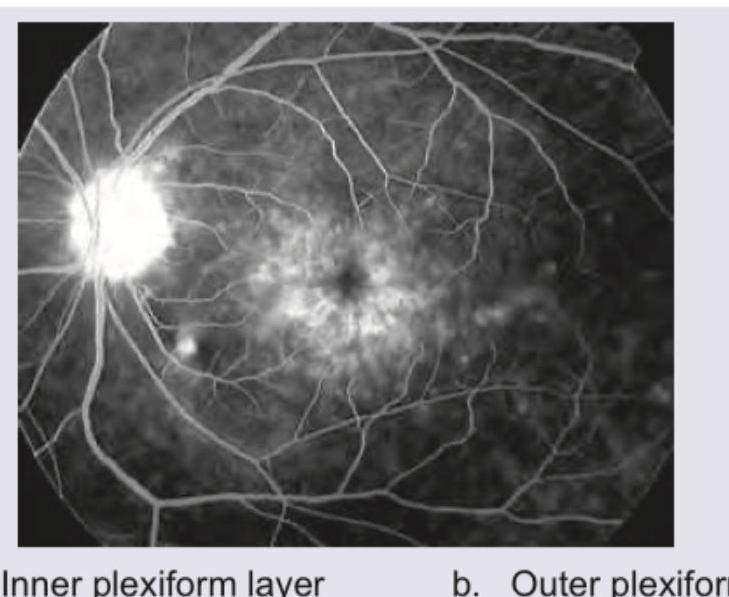
The given FFA appearance occurs due to accumulation of dye in which of the following layers of retina?
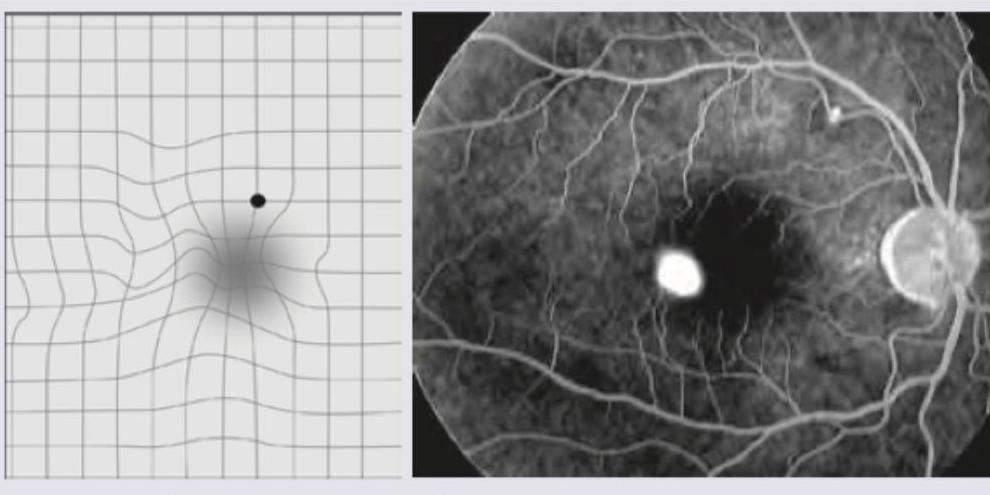
A 20-year-old college student has visual complaints represented in the image given below. FFA of the patient shows presence of:
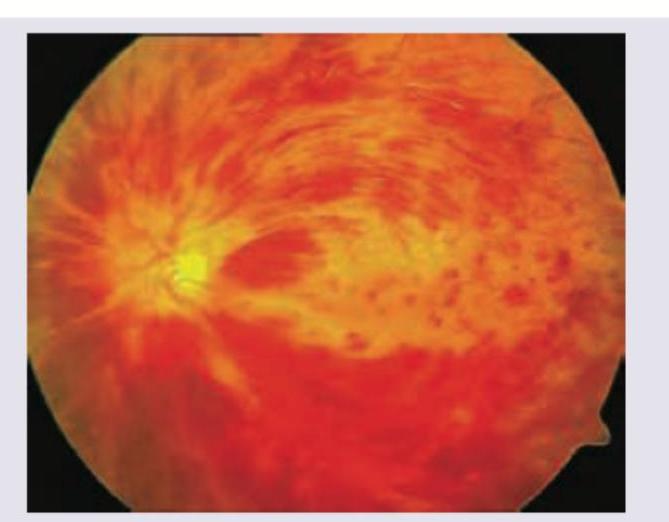
A 60-year-old polycythemia vera patient is having a marked reduction in visual acuity in both eyes. The fundus examination image is shown below. What is the most likely finding?
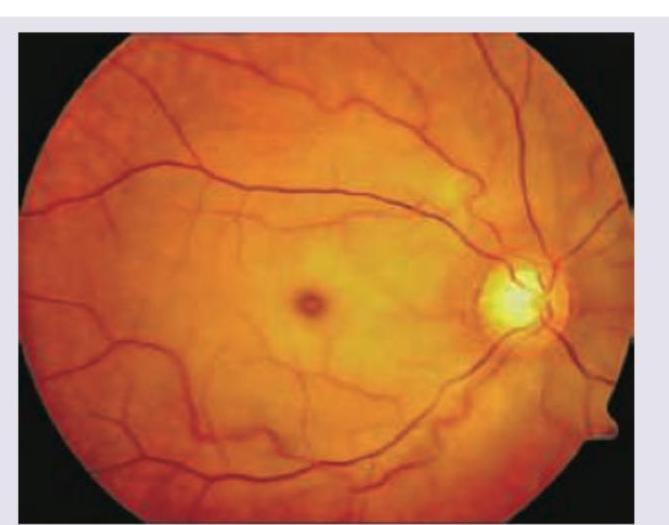
A 75-year-old patient with carotid artery bruit develops sudden onset, unilateral loss of vision. On examination direct pupillary light reflex is absent and visual acuity is profoundly reduced and a relative afferent pupillary defect is present. What does the given fundus examination show?
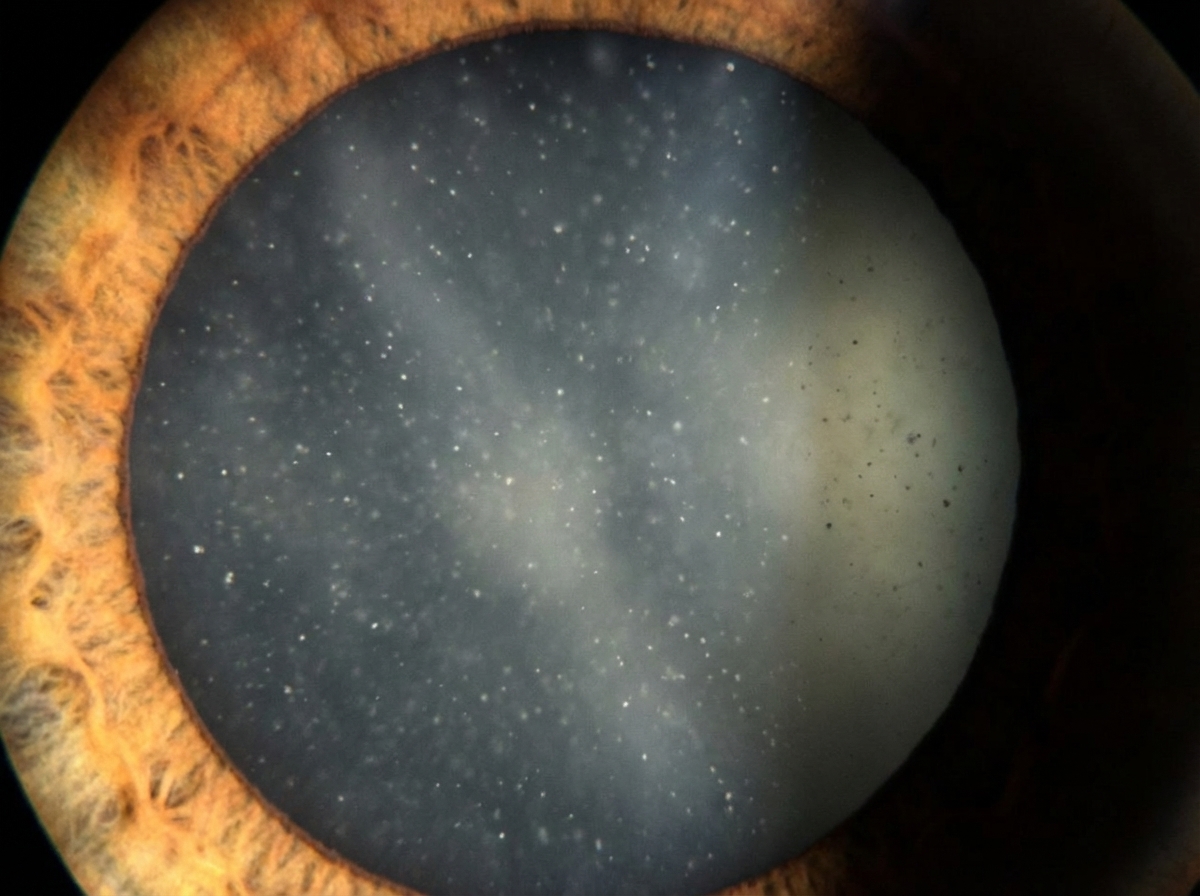
What does the following image show?
During annual medical check-up, a 55-year-old hypertensive corporate executive is found to have ophthalmoscopic findings as shown in the image given below. What is it composed of?
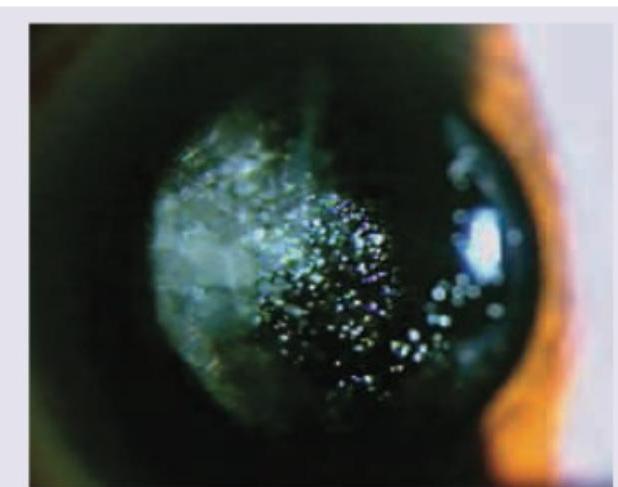
All of the following are responsible for the condition shown in the image except:

A 6-month-old child with retinoblastoma is brought with the following presentation in the right eye. The presentation shown is known as:
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app