
Diseases of the Retina — MCQs

On this page
What is incorrect about the disease shown below?
What is the fundus finding shown below?
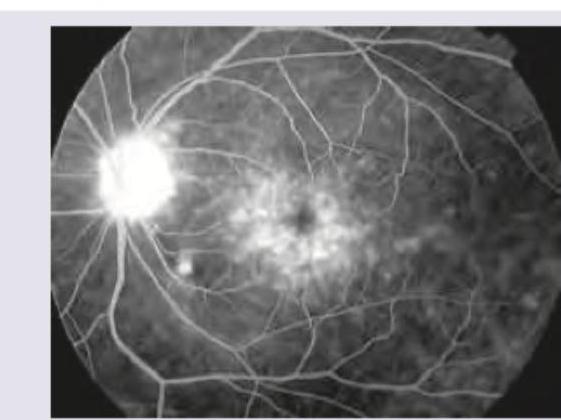
The FFA given below shows:
Identify the appearance:
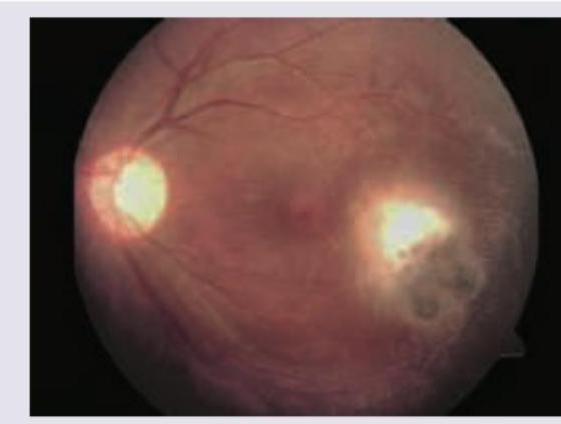
Identify the fundus appearance seen on examination:
The fundus shown below indicates presence of:
What pathology is shown in this fundus image?
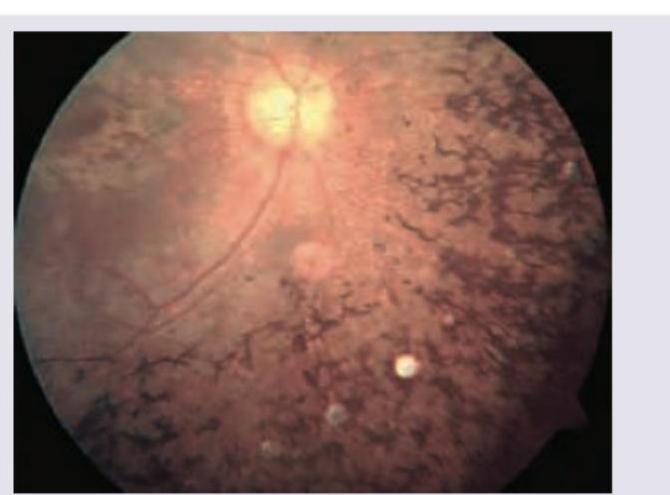
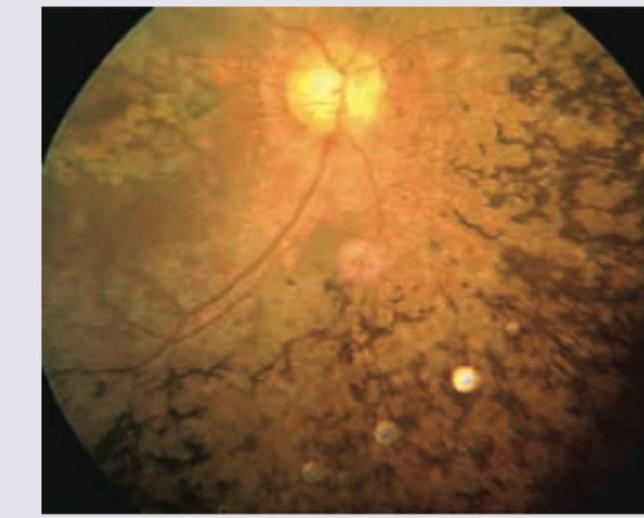
A 25-year-old male patient came with history of progressive night blindness and decreased vision since childhood. Now he has tubular vision. Retinal examination as shown below revealed jet black, spidery spots similar to bone corpuscles. Which of the following statements is true?
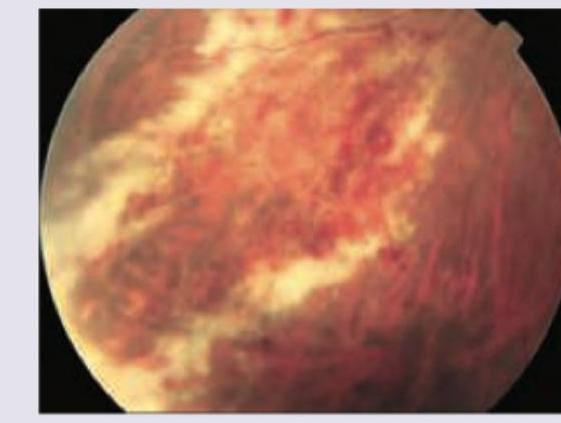
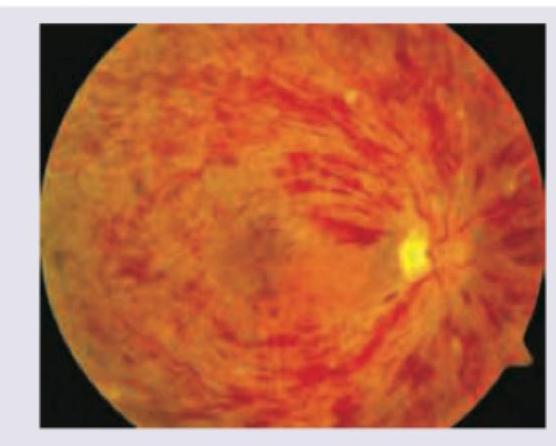
This is the picture of the fundus of a female patient, who was on estrogen containing pills, and presents with sudden deterioration of vision. What is the likely diagnosis?
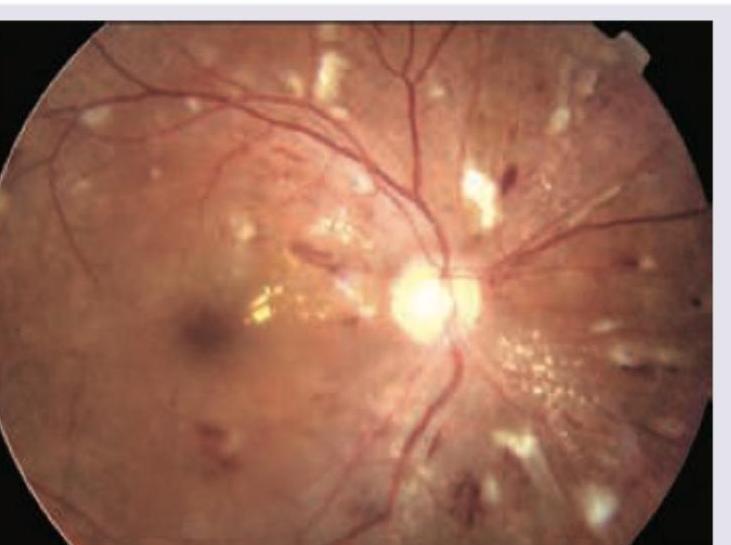
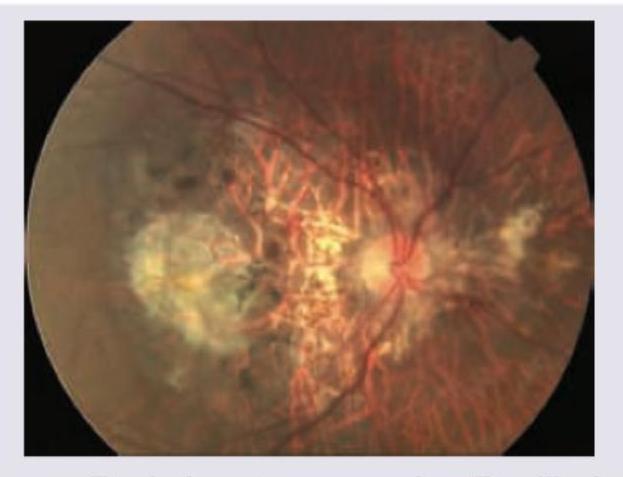
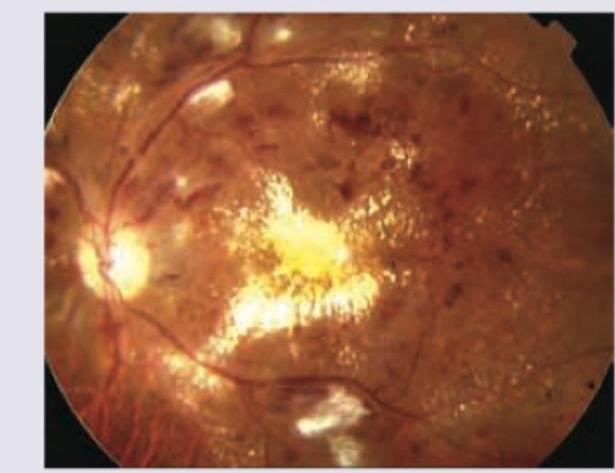
A 60-year-old patient during annual check-up had a report of HbA1C of $10 \%$. What stage of diabetic retinopathy is shown?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app