
Diseases of the Retina — MCQs

On this page
Which of the following is NOT a feature of diabetic nonproliferative retinopathy?
Lacquer cracks in pathological myopia are due to breaks in which layer?
A child presents with unilateral white reflex and raised intraocular pressure. What is the required investigation, excluding one option?
Which of the following conditions is associated with Macular edema?
Regarding Retinitis pigmentosa, which of the following statements is FALSE?
Bilateral retinoblastoma is ideally managed by which of the following except?
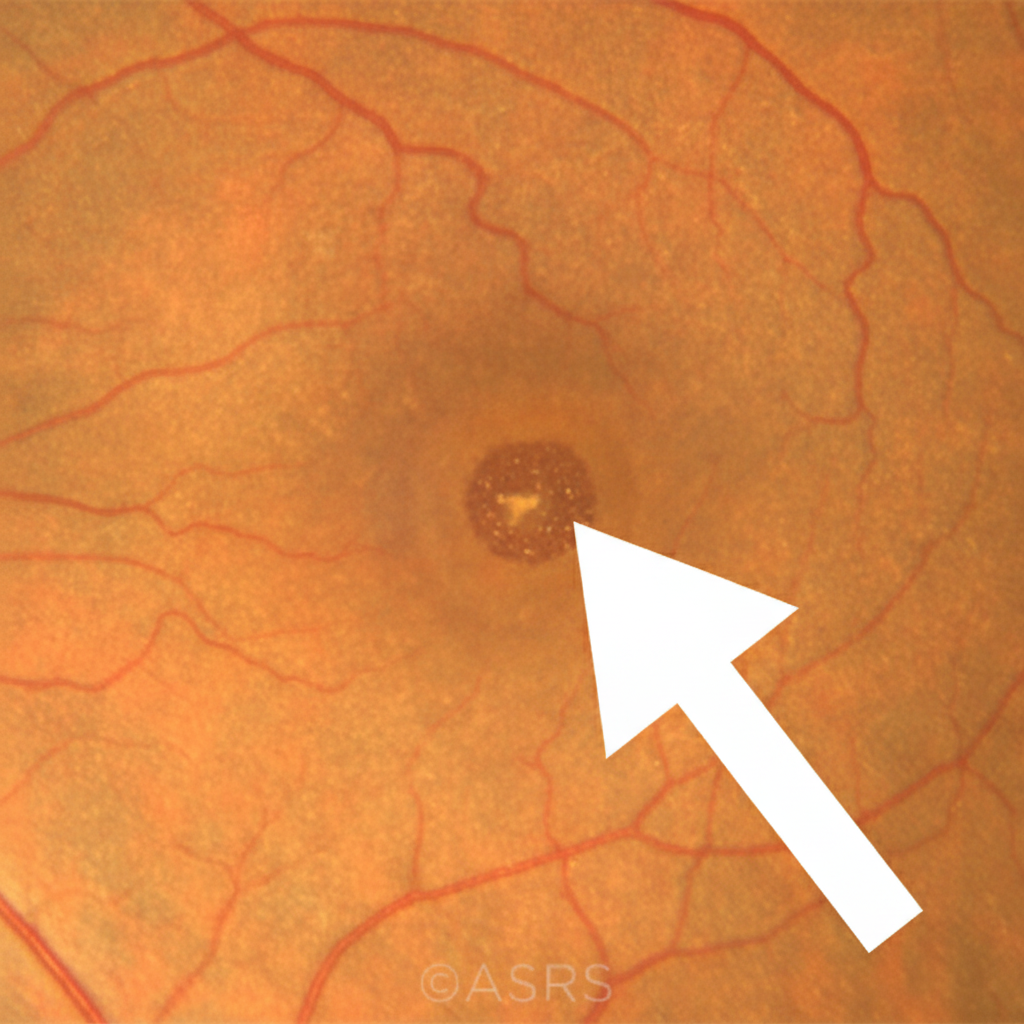
What finding in a fundus examination of a myopic patient is indicated by an arrow?
What is the cause of blindness in Central Retinal Vein Occlusion (CRVO)?
Malignant change in a choroidal nevus is evidenced by:
All of the following statements are true regarding indirect ophthalmoscopy, except:
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app