
Diseases of the Retina — MCQs

On this page
Angioid streaks occur in which of the following conditions?
Which of the following conditions can premature babies develop?
The "pizza pie" appearance of the retina is characteristic of which of the following conditions?
Hard exudates are not seen in which of the following conditions?
Rubeosis iridis is NOT COMMONLY seen in:
Roth's spots are seen in which of the following conditions?
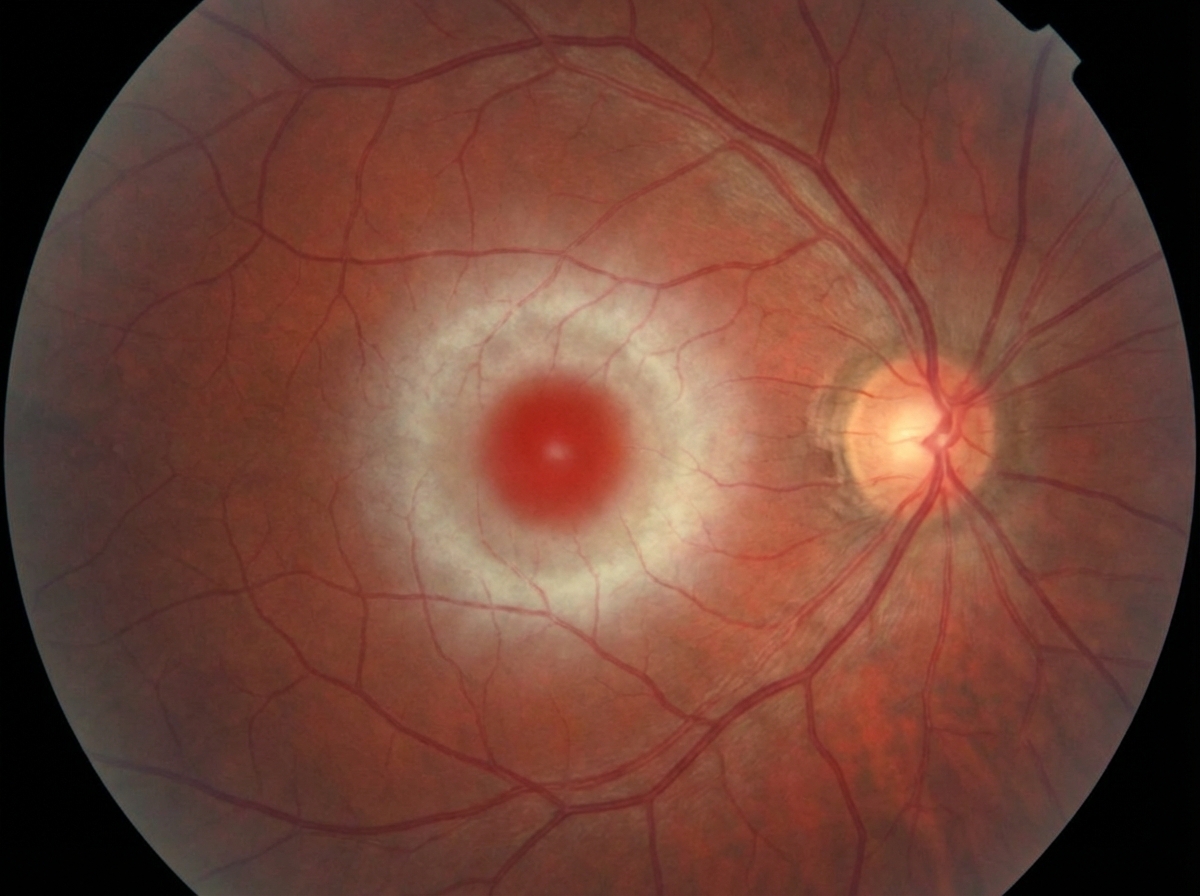
In which of the following diseases is the eye finding shown below seen?
What is true about Birdshot Chorioretinopathy?
Snow banking is typically seen in which of the following conditions?
Retinitis pigmentosa is associated with which of the following conditions, except?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app