
Diseases of the Retina — MCQs

On this page
A 47-year-old woman presents with accelerated hypertension (blood pressure 210/105 mm Hg) and frequent headaches for the past month. She has a past medical history notable for hypertension during her first pregnancy, and her family history is positive for hypertension in both parents and a brother. On physical examination, her blood pressure is 210/105 mm Hg in both arms, heart rate is 88/min, and she is alert and oriented. Cardiac examination reveals an S4, lungs are clear, and there are no focal neurological deficits. Which of the following findings are most likely on examination of the fundi?
Which of the following agents is NOT used in the treatment of Diabetic Macular Edema?
What is true regarding metamorphopsia?
What is the most common etiology of recurrent vitreous hemorrhage in a young patient?
'Bull's eye' lesion in the macular region is seen in which of the following conditions?
When should screening for Diabetic Retinopathy be initiated after the diagnosis of diabetes?
Exudative retinal detachment occurs in which of the following conditions?
What is the parasitic cause of uveitis?
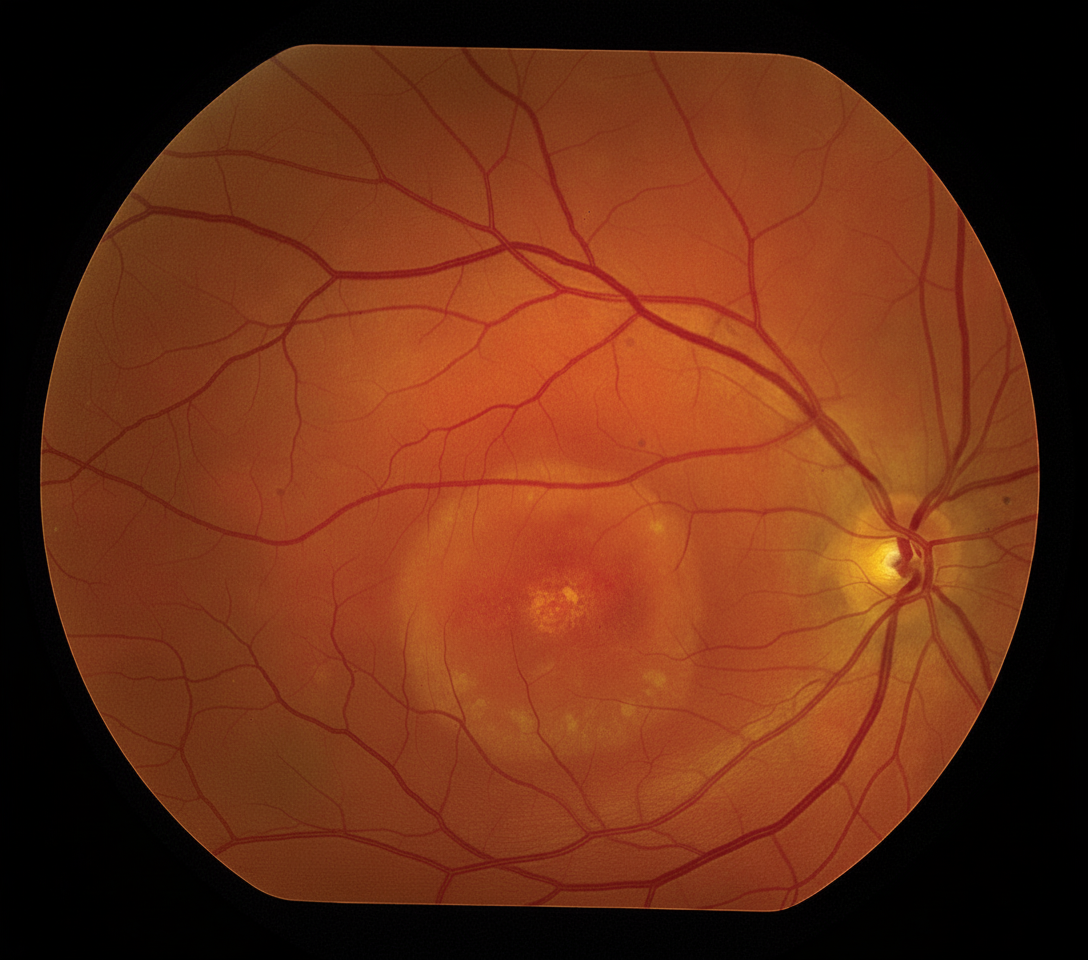
The fundus photograph shown is characteristic of which of the following conditions?
A 65-year-old man presents with metamorphopsia. On examination, he has yellow deposits subretinal near the macula in both eyes. The rest of the fundus is normal. What is the probable diagnosis?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app