
Diseases of the Retina — MCQs

On this page
Which of the following types of macular dystrophy is associated with the typical egg yolk lesion located in the central macula?
Which of the following is true about inverse Retinitis pigmentosa?
Which of the following statements is not true regarding rhegmatogenous retinal detachment?
Snowball opacities near the ora serrata are pathognomonic of which condition?
Which of the following conditions is characterized by a 'headlight in fog' appearance in the retina?
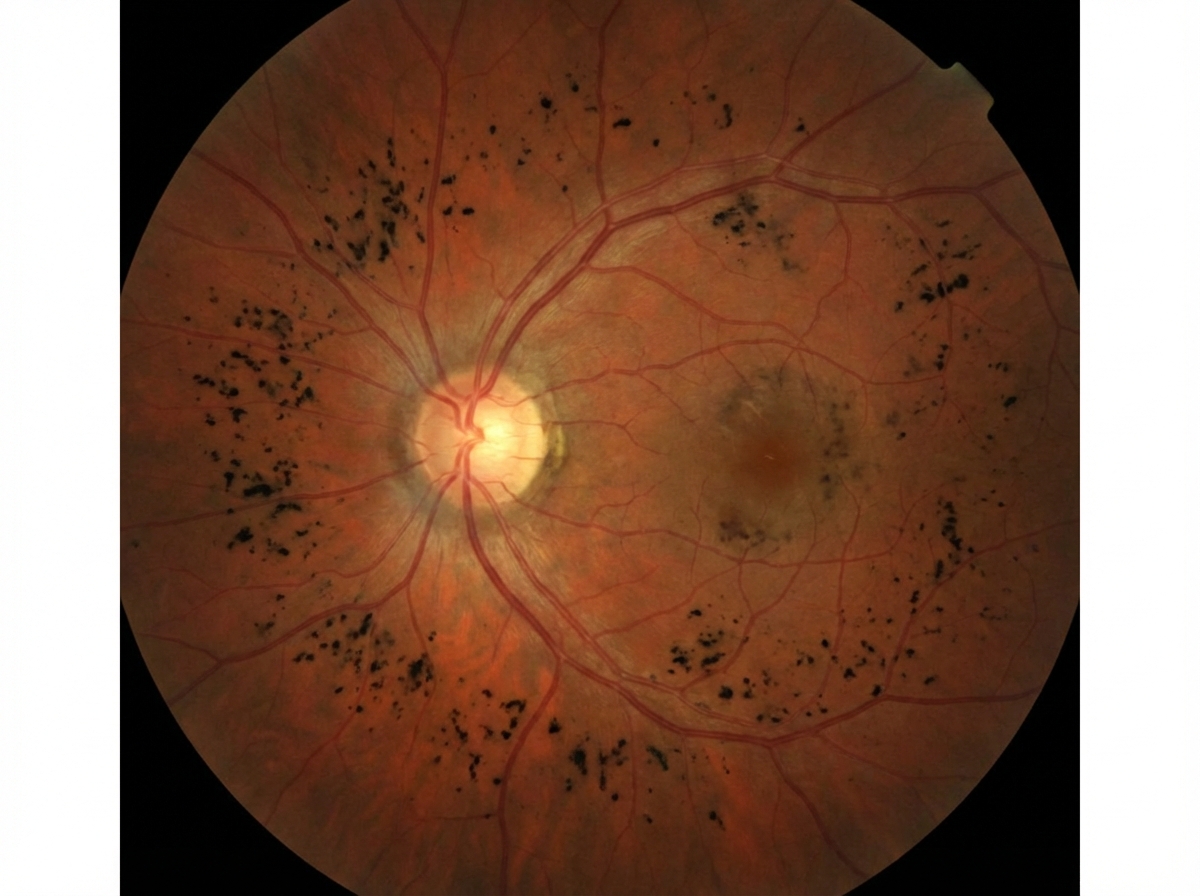
What is the following fundus finding shown below?
A cherry red spot on the retina is seen in which of the following conditions?
Floaters can be seen in all of the following conditions except:
Two tumours commonly associated with Masquerade syndrome are:
Tubular vision is seen in which condition?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app