
Diseases of the Retina — MCQs

On this page
All of the following are seen in retinitis pigmentosa except?
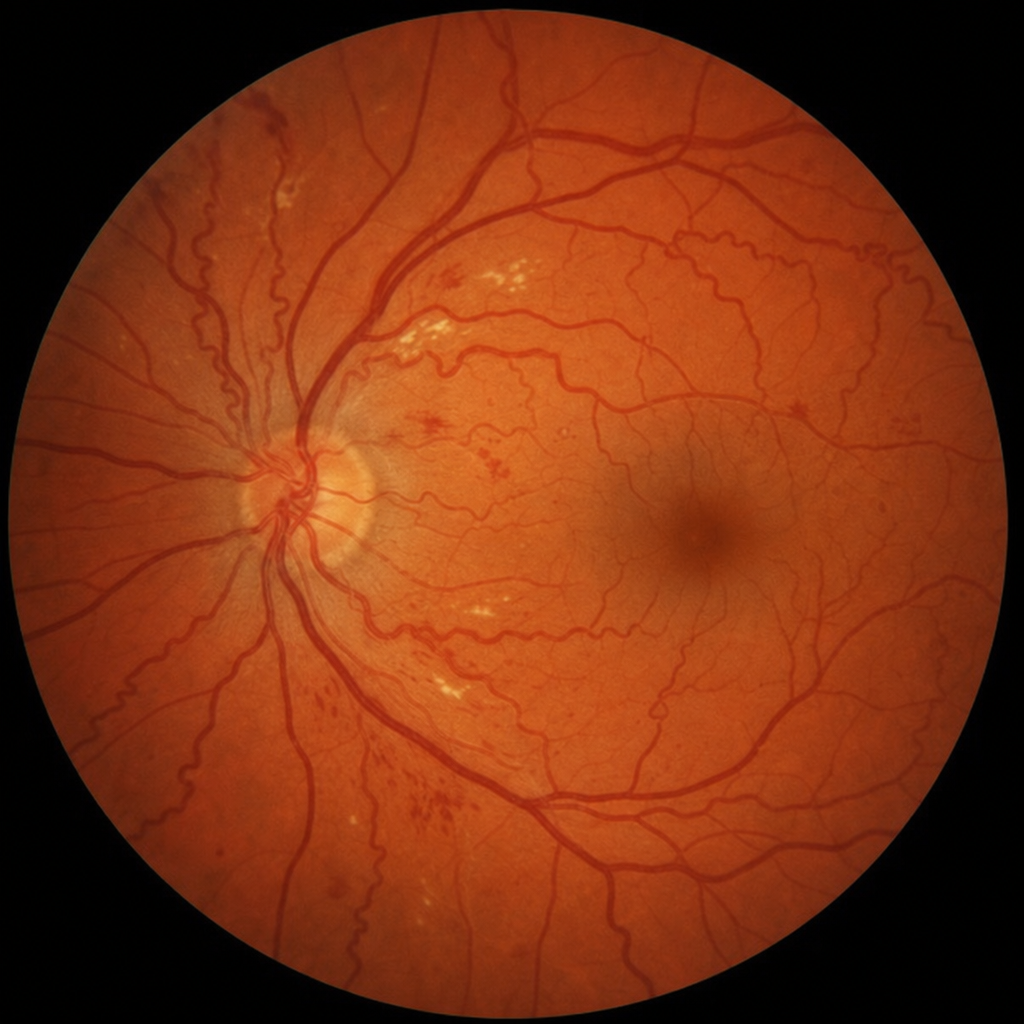
What is the diagnosis based on the following fundus examination?
Which of the following is NOT a recognized test for assessing macular function?
GNAQ mutations are seen in which of the following conditions?
All of the following are true about the electroretinogram (ERG) except:
Which of the following conditions is best investigated using angiography?
All of the following are true about retinoblastoma except:
A patient with Coats' disease presents with leukocoria. What condition needs to be differentiated from this?
A "white centered retinal haemorrhage" is seen in which of the following conditions?
Which of the following is NOT a layer of the retina?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app