
Diseases of the Retina — MCQs

On this page
CRAO may be seen in which of the following conditions?
Which of the following is NOT a differential diagnosis of Retinoblastoma?
In central serous retinopathy, which of the following is true?
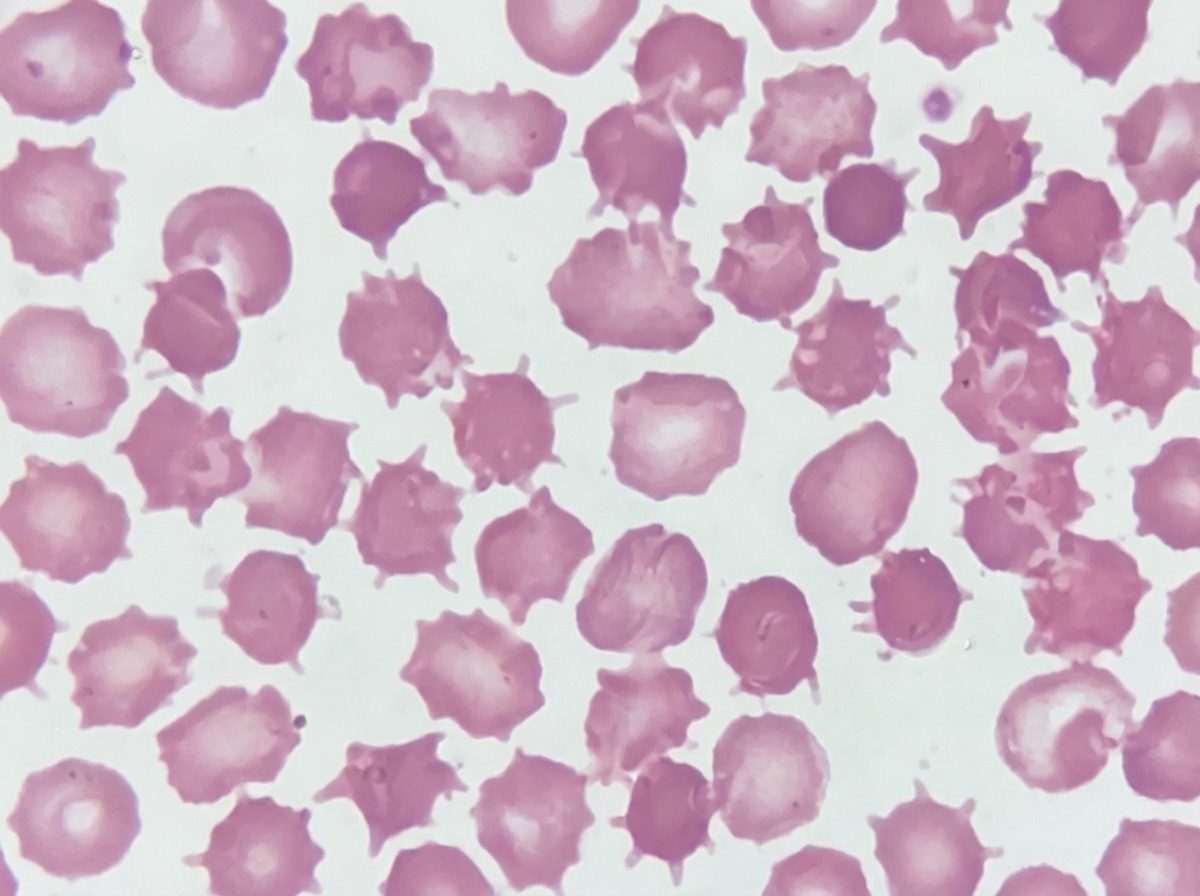
A 6-year-old male presents with steatorrhea, failure to thrive, and ataxia. Blood smear examination reveals acanthocytes, and labs show markedly reduced LDL and apolipoprotein B. Which of the following ocular conditions is most likely to be associated with this patient?
A 40-year-old male with diabetes mellitus presents with vitreous hemorrhage. What is the most important cause for it?
Soft exudates are found in all of the following conditions except?
Dot and blot hemorrhages and flame-shaped hemorrhages can be characteristically seen in which of the following conditions?
The mother of a one and a half year old child gives history of a white reflex from one eye for the past 1 month. On computed tomography scan of the orbit, there is calcification seen within the globe. What is the most likely diagnosis?
All of the following are true about central retinal artery occlusion (CRAO) except:
Angioid streaks are seen in which of the following conditions?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app