
Diseases of the Retina — MCQs

On this page
Which imaging modality is best for evaluating retinoblastoma?
A 75-year-old patient with a 25-year history of diabetes mellitus presented with sudden painless loss of vision. Fundus examination revealed flame-shaped hemorrhages in the retina. What is the probable diagnosis?
In cystoid macular edema, what is the basic defect?
What is the most constant and critical finding in retinitis pigmentosa?
Which disease, caused by a mutation in the BEST1 (VMD2) gene, is best diagnosed by a pathological test?
All of the following may be associated with night-blindness except?
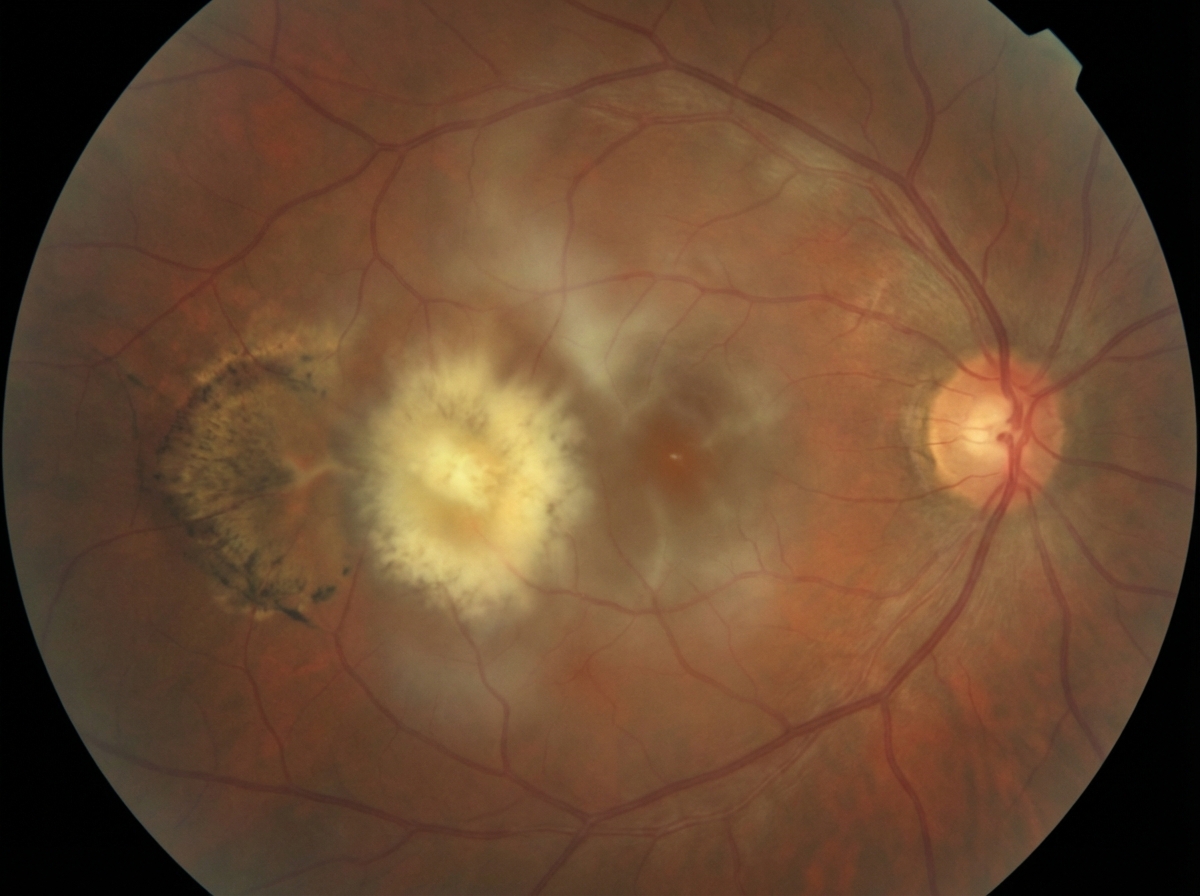
What is the best management for an immunocompromised patient with the following fundus findings?
Which of the following agents is not used in the treatment of Diabetic Macular Edema/Retinopathy?
What percentage of retinoblastomas are bilateral?
A lesion is identified in the orbit. What is the most likely diagnosis?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app