
Diseases of the Retina — MCQs

On this page
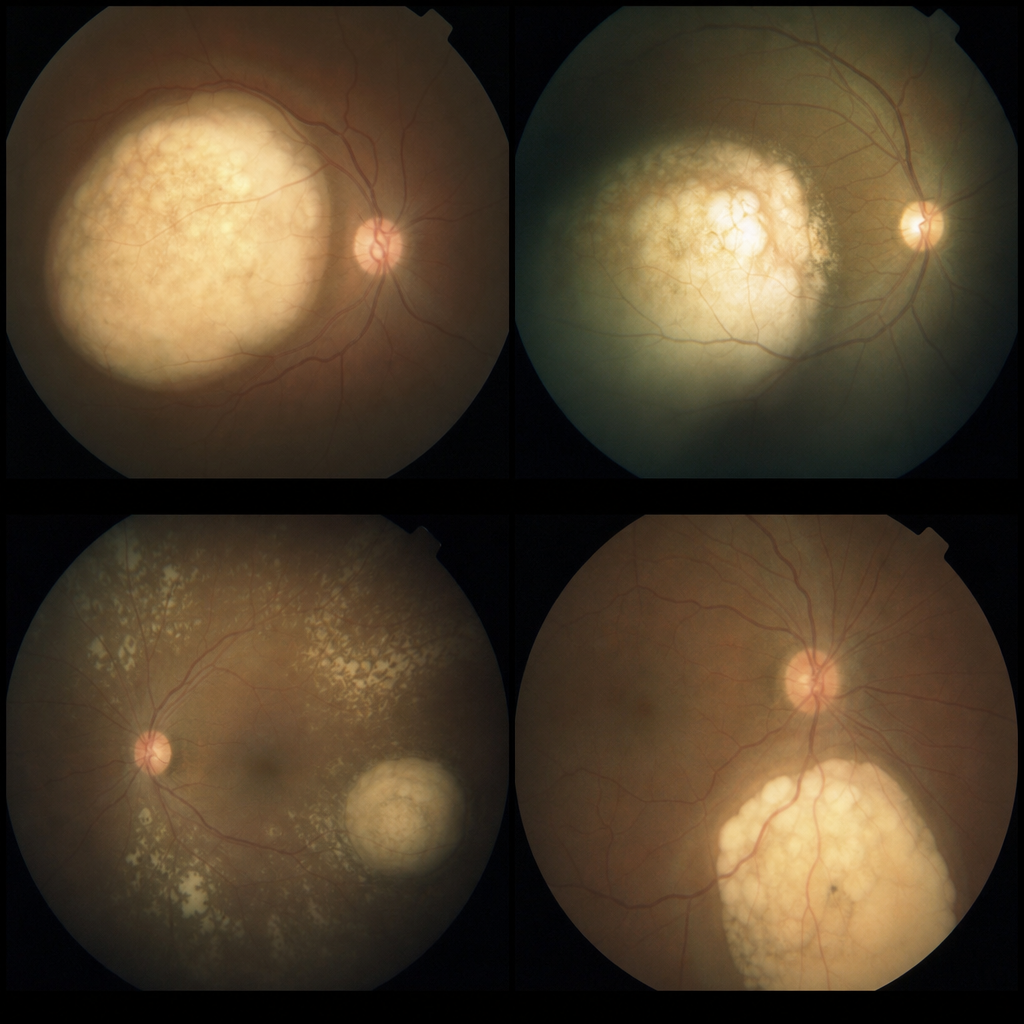
Angiography of choroidal melanoma shows which of the following appearances?
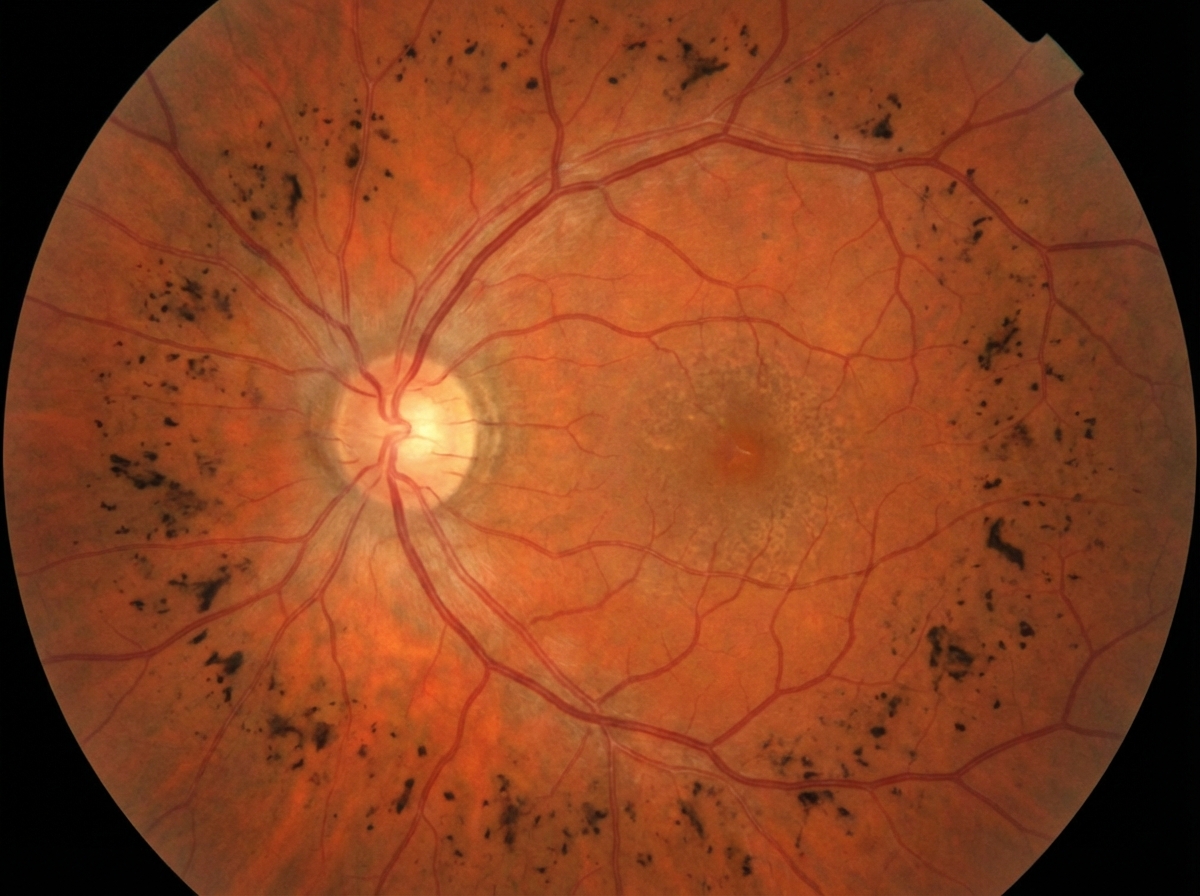
Which condition is characterized by the presented fundus findings?
A premature infant is delivered at 27 weeks of gestation and weighs 1500 gm. At what point should a fundus examination by an ophthalmologist be requested?
What is the most common presentation of Retinoblastoma?
What is the most characteristic finding of retinitis pigmentosa?
Dark adaptation is delayed in all of the following conditions except:
What is the strongest force of bonding between the retina and the retinal pigment epithelium (RPE)?
A diabetic patient is at greatest risk of developing which of the following types of retinal detachment?
Loss of vision may occur due to occlusion of which artery?
A 2-year-old child presents with leukocoria in one eye. Examination reveals a unilateral Group D retinoblastoma (International Classification of Retinoblastoma) with retained visual potential and no high-risk features such as anterior chamber involvement, neovascular glaucoma, or optic nerve involvement. What is the primary treatment?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app