
Age-Related Macular Degeneration — MCQs

In diabetic retinopathy, which layer of the retina is primarily affected?
Assertion: Vitamin D analogues are effective in psoriasis. Reason: They reduce keratinocyte proliferation
A patient presents with a central scotoma and metamorphopsia. What is the most likely cause?
Most common age related change in vitreous?
Fluorescein dye for ophthalmological diagnosis is injected into:
SAFE strategy is recommended for-
What type of deposit is commonly associated with age-related macular degeneration?
In the context of ophthalmology, the Amsler grid is primarily used for:
Ranibizumab is a monoclonal antibody against?
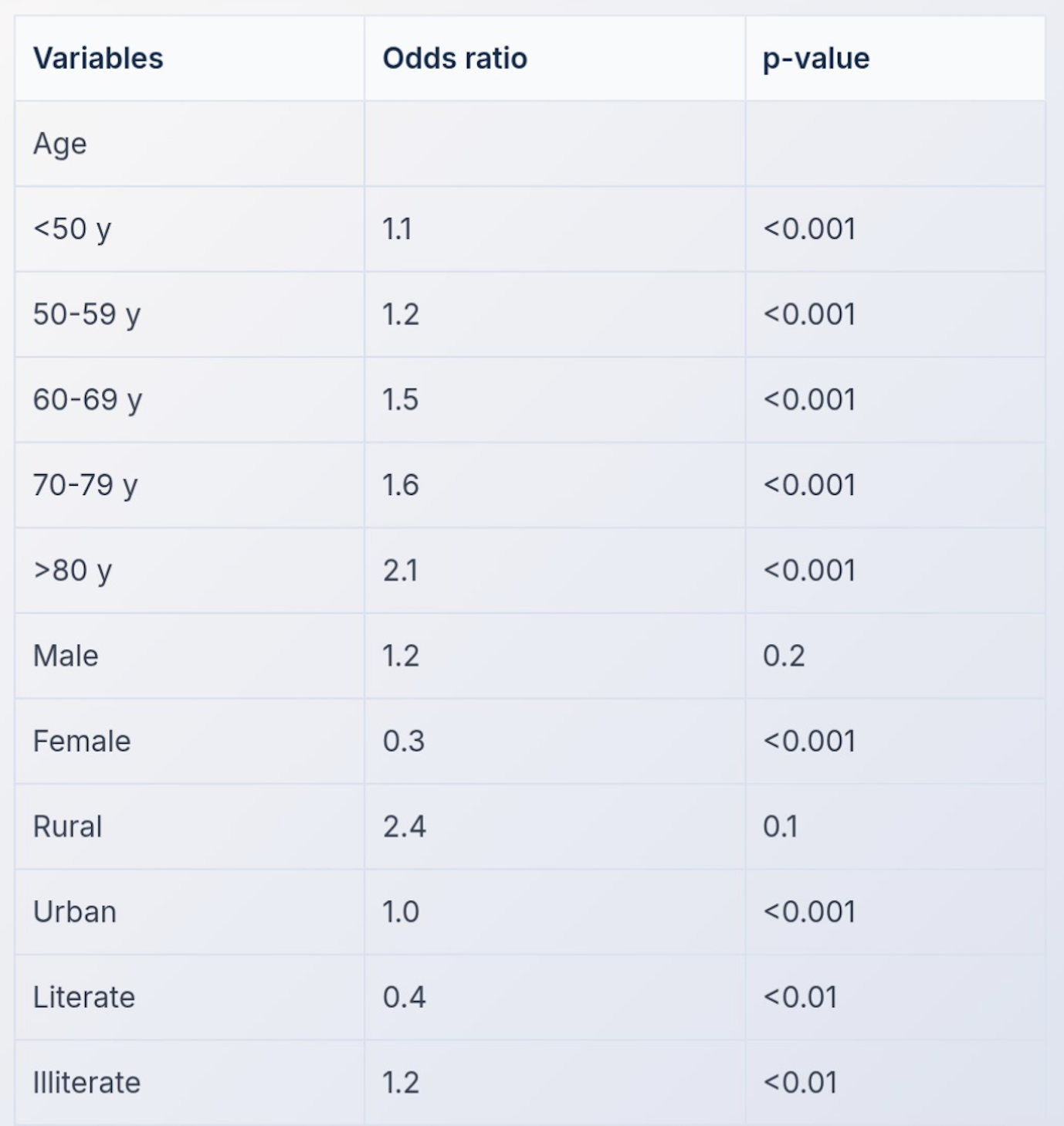
A multivariate analysis was conducted to examine the relationship between risk of developing blindness and age. The results are shown in the table below. Which of the following is true?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app