
Diseases of the Retina — MCQs

On this page
. A patient presented with sudden loss of vision with the retinal findings as shown in the image. What is the most probable diagnosis?
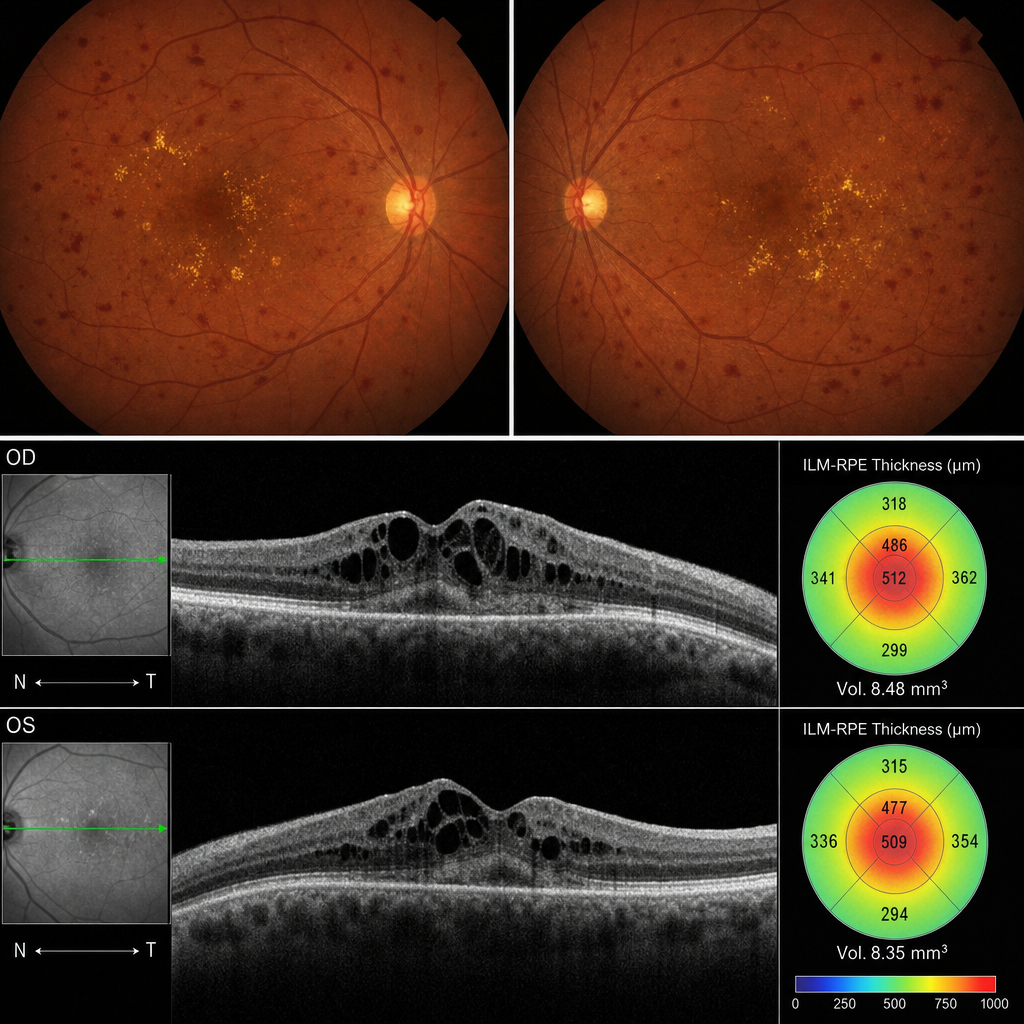
A 52-year-old woman with a 15-year history of poorly controlled type 2 diabetes mellitus presents with gradual blurring of central vision in both eyes over the past 6 months. Her HbA1c is 10.2%. Fundus examination reveals dot-blot haemorrhages and hard exudates in the macular region bilaterally. Her best-corrected visual acuity is 6/24 in the right eye. The OCT is shown (Image 2). According to current evidence-based guidelines, which of the following represents the most appropriate first-line treatment for the condition demonstrated on imaging in this eye?
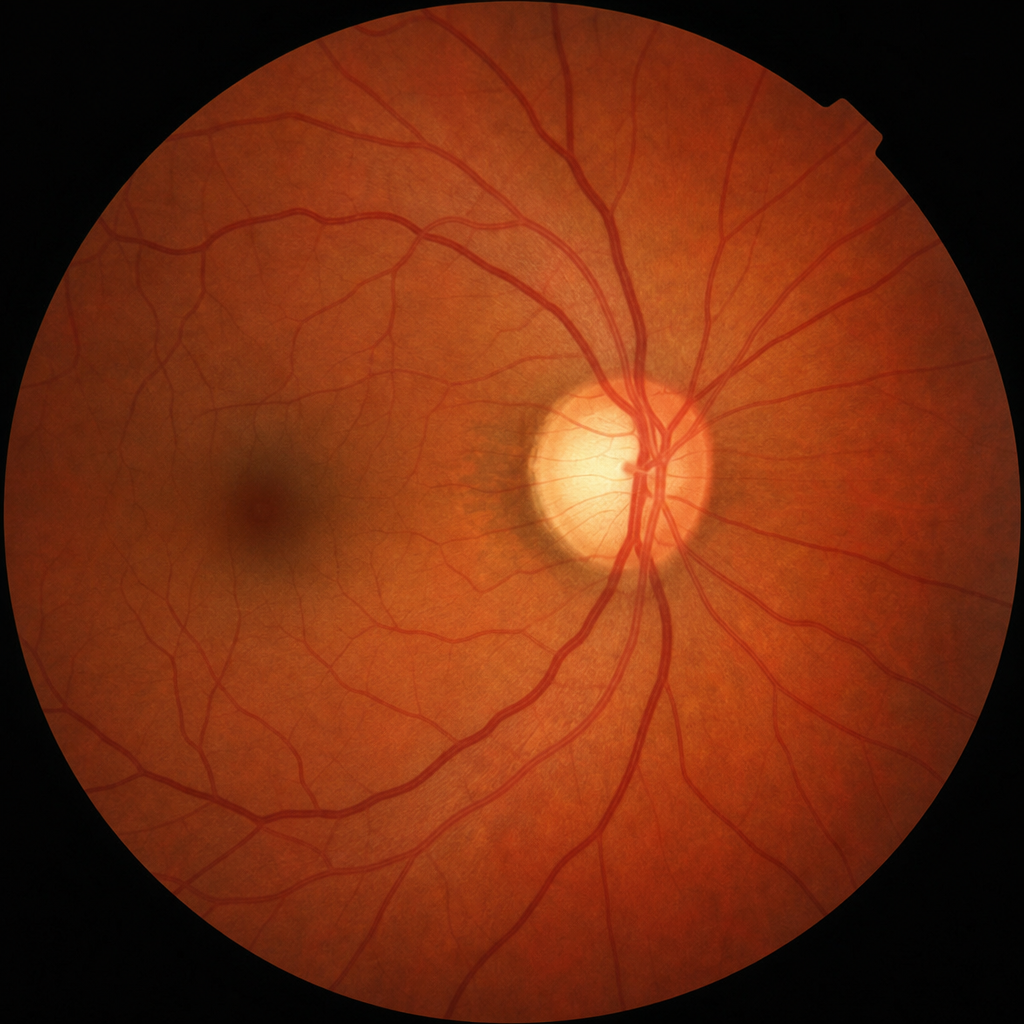
A 62-year-old man with a family history of glaucoma attends a routine eye clinic. He reports no visual symptoms. Intraocular pressure is 26 mmHg in the right eye. Gonioscopy reveals an open angle. The appearance of the right-eye optic disc is shown in Image 2 (standard fundus orientation: superior disc pole at top, inferior disc pole at bottom, nasal side to the right). Automated perimetry reveals an arcuate scotoma in the superior field. Which of the following best describes the structural finding visible in the image that accounts for this visual field loss?
The outer blood-retinal barrier is formed by which structure?
About retinitis pigmentosa, all are true EXCEPT?
In cystoid macular edema, fluid collects in the macular region at the level of which layer?
Waves present in electroretinogram are all EXCEPT:
Which of the following is not a high-risk characteristic in proliferative diabetic retinopathy?
A 60-year-old man with a 10-year history of hypertension and diabetes mellitus presents with reduced vision in one eye. Fundus examination reveals a central bleed, while the fellow eye is normal. What is the most likely diagnosis?
Examination of the vitreous is best performed by which of the following methods?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app