
Diseases of the Lens — MCQs

On this page
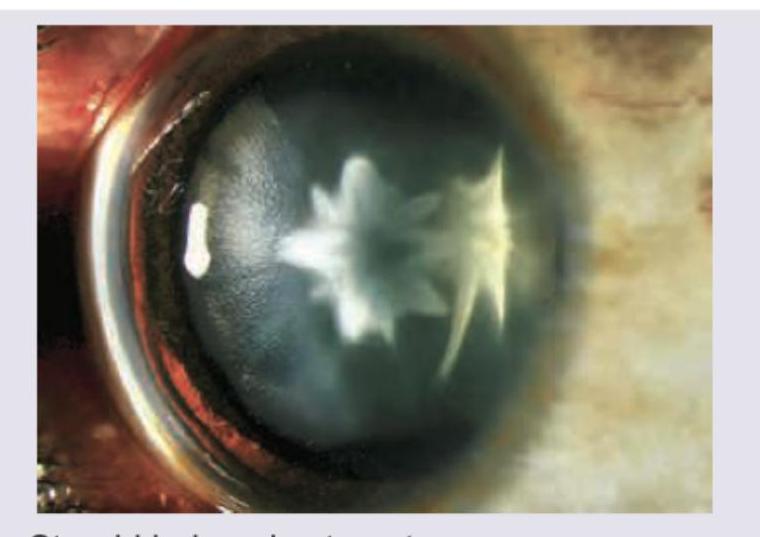
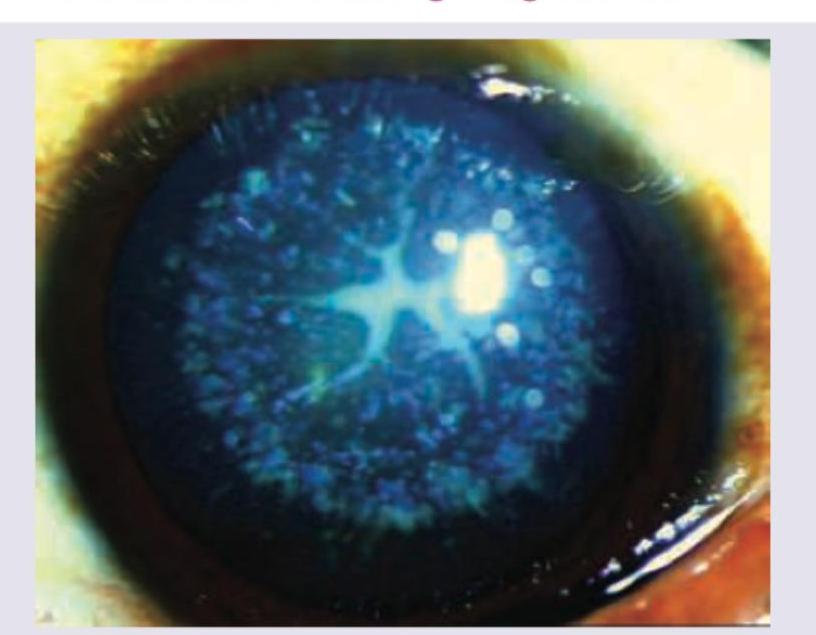
The presentation shown below is seen in:
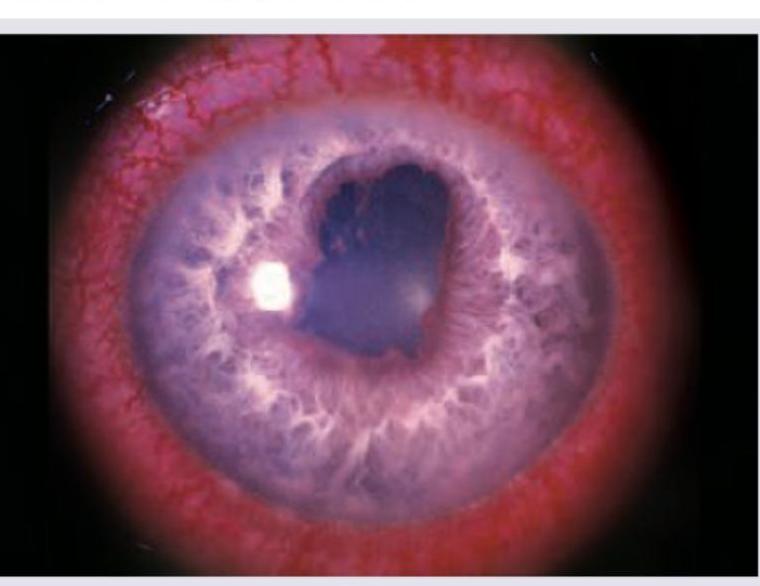
A patient presents with pain, redness, and photophobia. The slit-lamp image is shown below. What is the diagnosis?
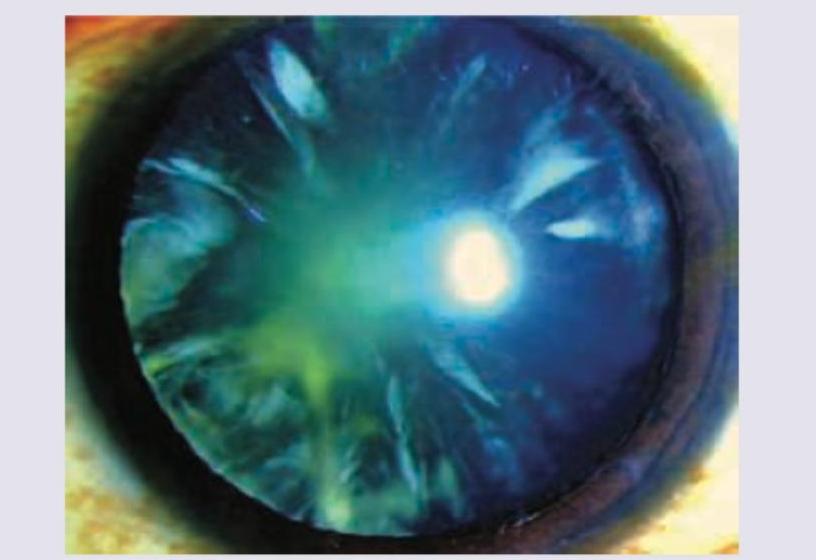
Which type of cataract is shown in the image?

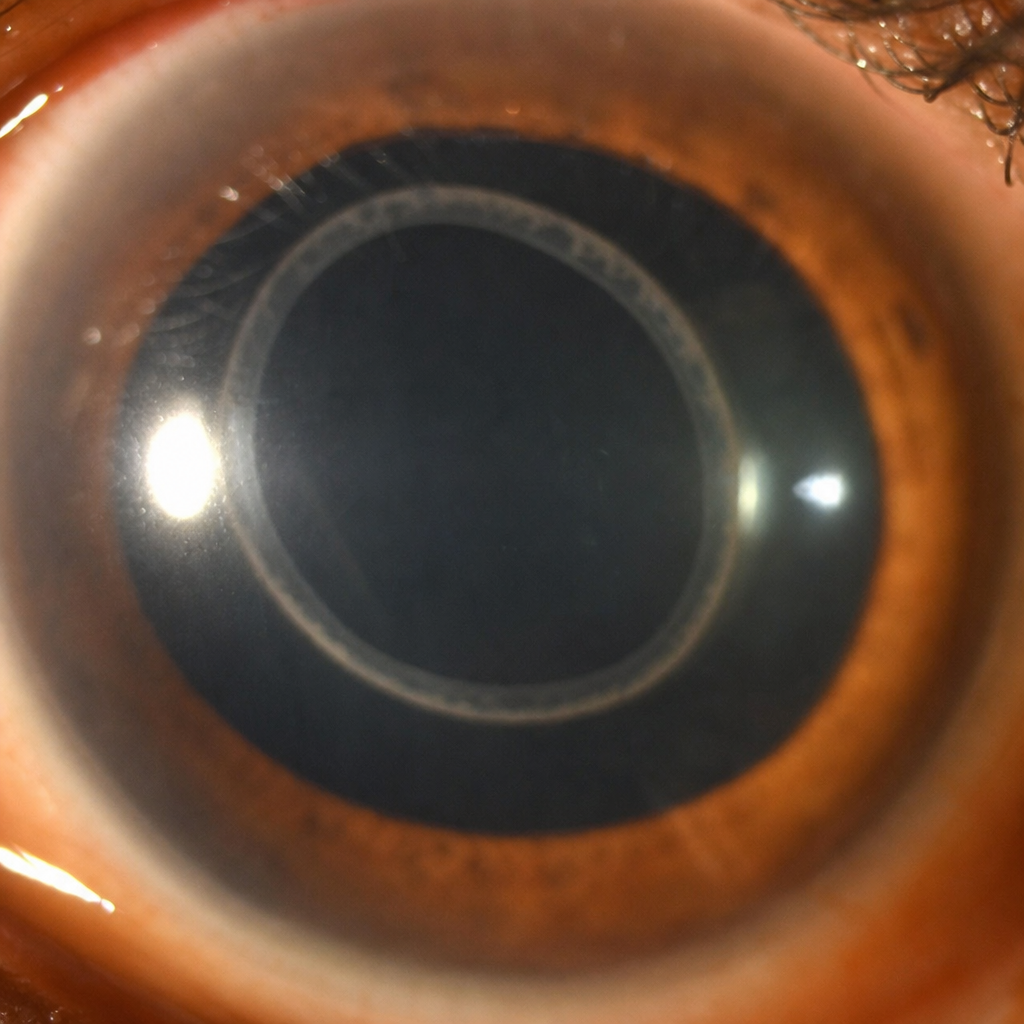
What does the following image show?
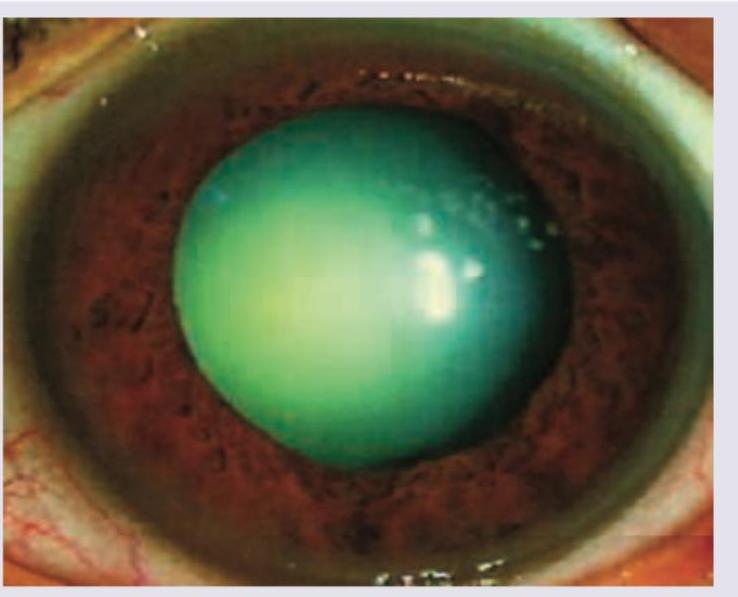
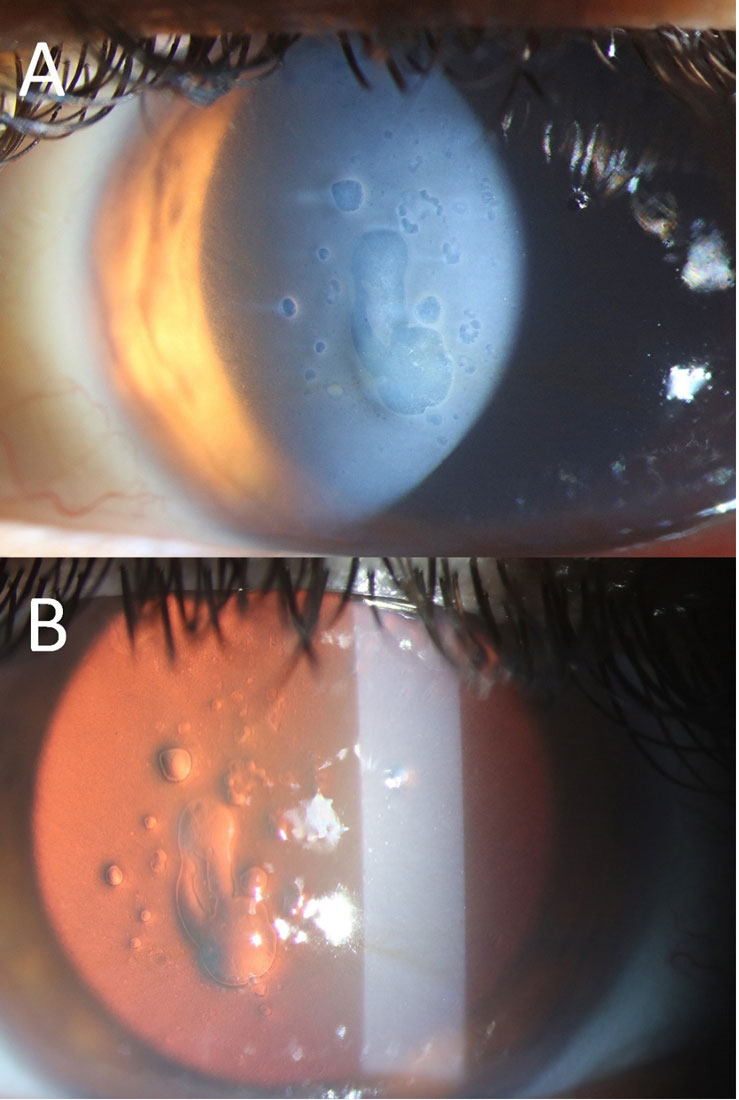
A 55-year-old banker presents with painless progressive loss of vision. He also complains of glare at night especially when driving back home. Recently his wife commented on the whiteness in his eye. What does the image show?
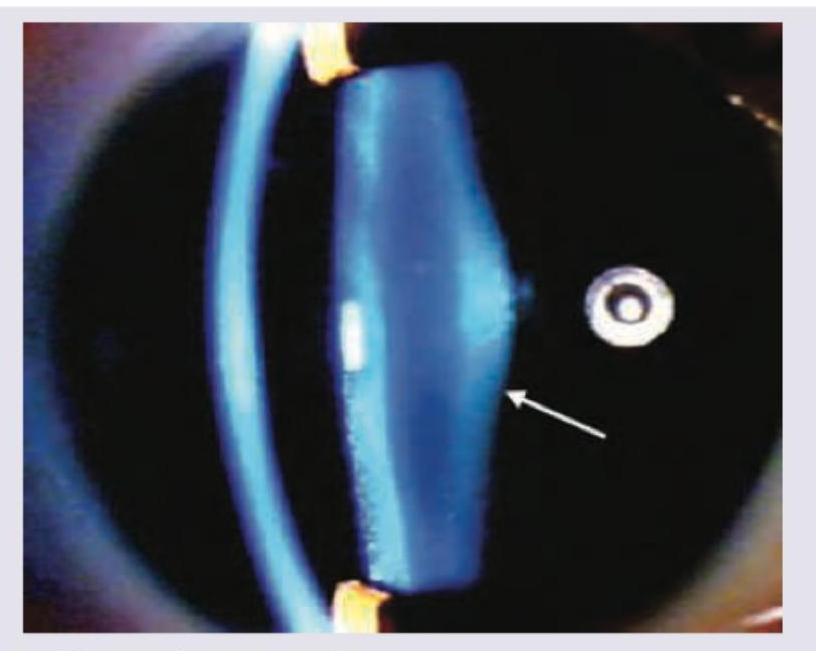
What does the following image show?
What does the following image show?
What does the following image show?
A patient, three years after cataract extraction with intraocular-lens implantation, presents with the condition shown in the image and complains of decreased vision. What is the most likely diagnosis?
Rosette cataract is seen after:
Practice by Chapter
Lens Anatomy and Physiology
Practice Questions
Age-Related Cataract
Practice Questions
Congenital and Developmental Cataracts
Practice Questions
Traumatic Cataract
Practice Questions
Metabolic Cataracts
Practice Questions
Drug-Induced Cataracts
Practice Questions
Cataract Surgery Techniques
Practice Questions
Intraocular Lens Implants
Practice Questions
Complications of Cataract Surgery
Practice Questions
Posterior Capsular Opacification
Practice Questions
Lens Subluxation and Dislocation
Practice Questions
Specialty IOLs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app