
Diseases of the Lens — MCQs

On this page
Acquired blue blindness is a feature of which of the following?
Which is the best intraocular lens (IOL) position?
The early changes in corticosteroid-induced cataract are in the form of:
What causes a 'Rosette cataract'?
Type of cataract in chalcosis is
A 32-year-old patient presents with blurred vision, photophobia, and mild ocular pain. Examination reveals aqueous flares and keratic precipitates in the anterior chamber. What is the likely diagnosis?
A 45-year-old patient with eye examination findings of a deep anterior chamber and jet-black pupil is prescribed +12D glasses. Likely diagnosis?
A 70-year-old patient who has been using presbyopia glasses for the past few years can now read the newspaper comfortably without the glasses. What is the most likely diagnosis?
An elderly patient presents with white, dandruff-like deposits on the anterior lens surface, seen during slit-lamp examination. What is the most likely diagnosis?
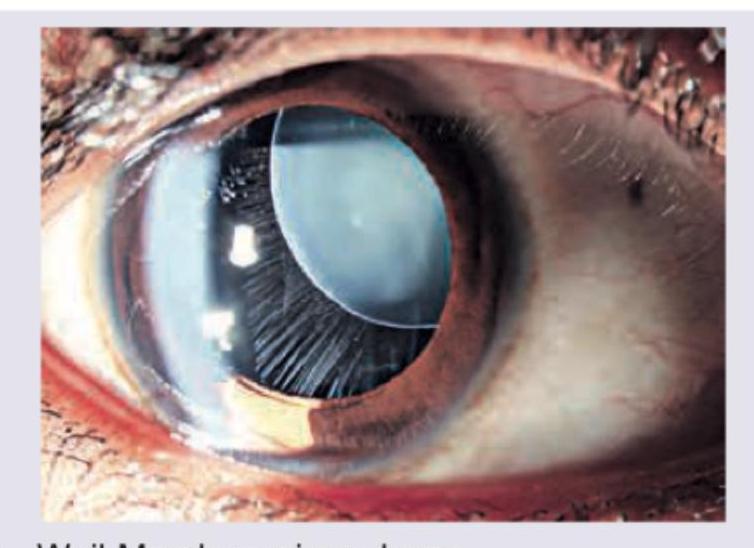
A short stature patient presents with the following presentation. Diagnosis is:
Practice by Chapter
Lens Anatomy and Physiology
Practice Questions
Age-Related Cataract
Practice Questions
Congenital and Developmental Cataracts
Practice Questions
Traumatic Cataract
Practice Questions
Metabolic Cataracts
Practice Questions
Drug-Induced Cataracts
Practice Questions
Cataract Surgery Techniques
Practice Questions
Intraocular Lens Implants
Practice Questions
Complications of Cataract Surgery
Practice Questions
Posterior Capsular Opacification
Practice Questions
Lens Subluxation and Dislocation
Practice Questions
Specialty IOLs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app