
Diseases of the Cornea — MCQs

On this page
Which of the following statements is NOT true regarding the corneal stroma?
All of the following conditions result in loss of corneal sensations except?
Corneal deposits are seen in all except?
A patient develops red eye two days after an episode of malaria. What is the probable cause?
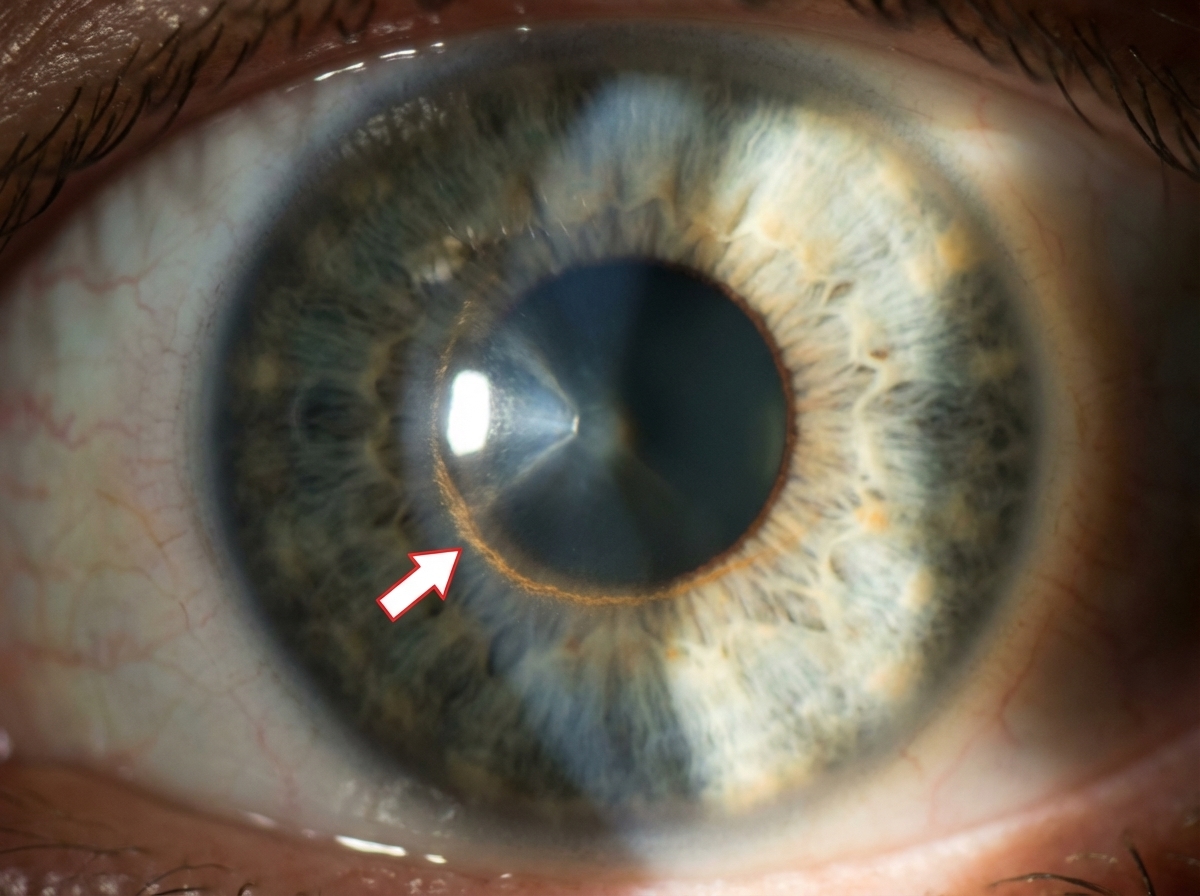
A Fleischer ring is a distinct feature of which of the following conditions?
A 30-year-old male presents with a 10-day history of decreased vision in his left eye. He reports trauma to the left eye with vegetative matter 10-15 days prior. Examination reveals an ulcerative corneal lesion with a raised, creamy infiltrate at the base. The ulcer margin is feathery and shows hyphae, with a few satellite lesions present. What is the most probable etiological agent?
Keratoconus is seen in which of the following conditions?
All of the following drugs are associated with corneal deposition except?
What is the characteristic feature of Herpes Simplex Keratitis?
The arrow marked sign is due to deposition of which substance?
Practice by Chapter
Corneal Anatomy and Physiology
Practice Questions
Bacterial Keratitis
Practice Questions
Viral Keratitis
Practice Questions
Fungal Keratitis
Practice Questions
Protozoan Keratitis
Practice Questions
Corneal Degenerations
Practice Questions
Corneal Dystrophies
Practice Questions
Keratoconus and Ectatic Disorders
Practice Questions
Corneal Transplantation
Practice Questions
Corneal Topography and Imaging
Practice Questions
Dry Eye Disease
Practice Questions
Corneal Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app