
Diseases of the Cornea — MCQs

On this page
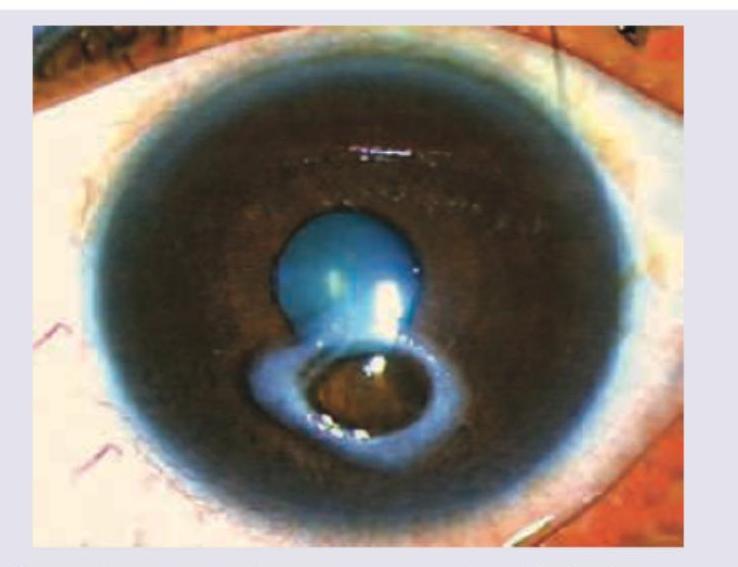
An 18-year-old male presents with complaints of acute pain and redness in the right eye with reduced visual acuity and a white spot on the cornea. What does the given ocular examination reveal?
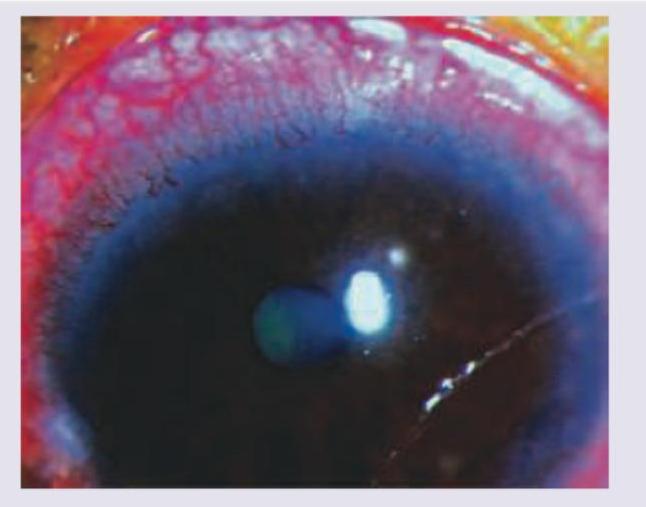
What does the following image show?
Identify the stain instilled in the eye in the following image:
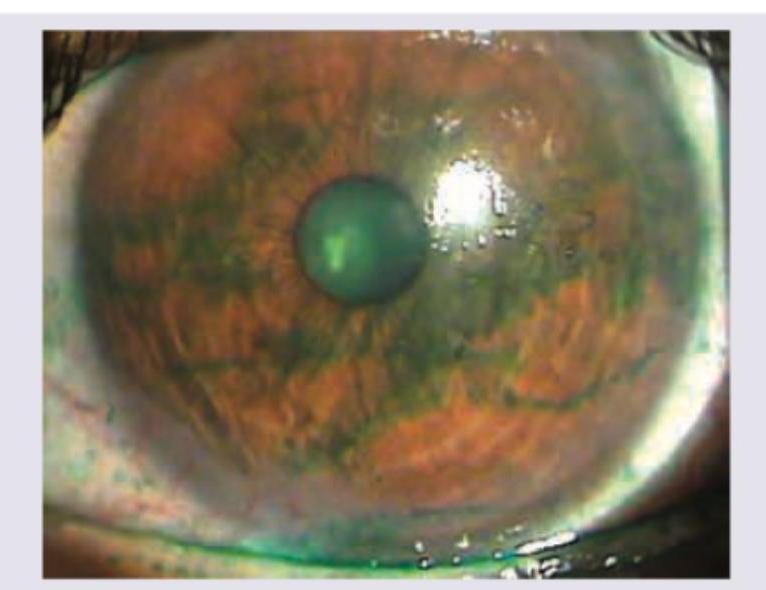
Which of the following is correct about the image shown? (Recent NEET Pattern 2016-17)
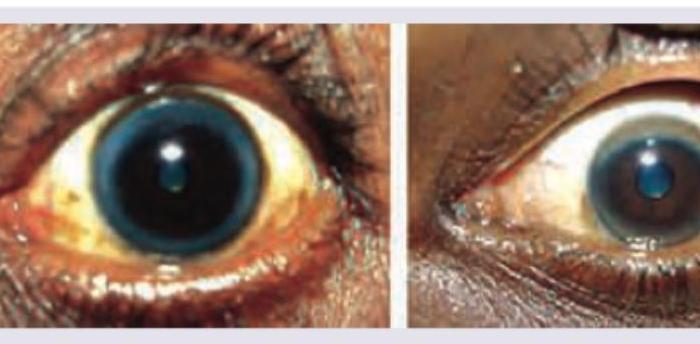
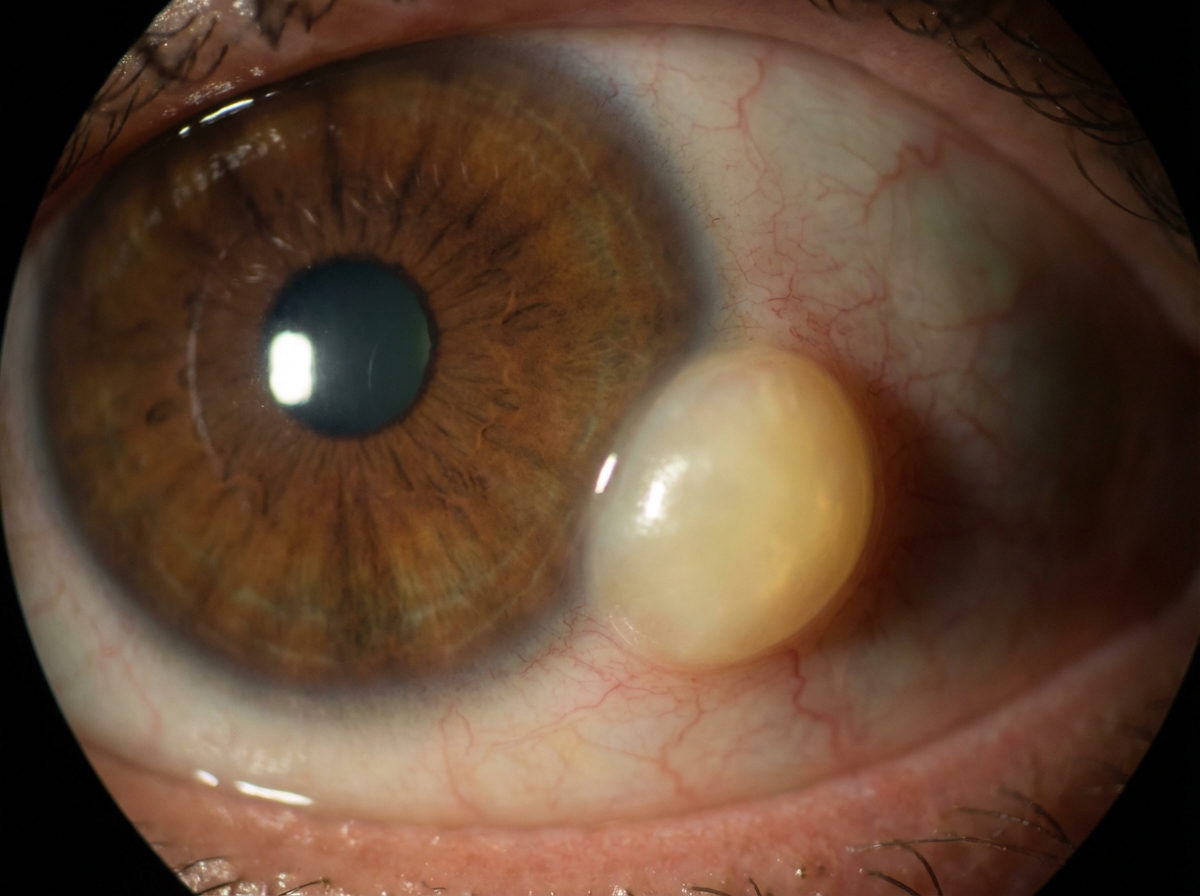
A patient presents to the OPD with the finding shown in the image. What is the most likely diagnosis?
Which of the following is not a feature of keratoconus?
Fleischer's ring is seen in?
True about Mooren's ulcer:
Cornea derives its nutrition chiefly from:
In uveitis, site of keratic precipitate is:
Practice by Chapter
Corneal Anatomy and Physiology
Practice Questions
Bacterial Keratitis
Practice Questions
Viral Keratitis
Practice Questions
Fungal Keratitis
Practice Questions
Protozoan Keratitis
Practice Questions
Corneal Degenerations
Practice Questions
Corneal Dystrophies
Practice Questions
Keratoconus and Ectatic Disorders
Practice Questions
Corneal Transplantation
Practice Questions
Corneal Topography and Imaging
Practice Questions
Dry Eye Disease
Practice Questions
Corneal Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app